

This list of 40 questions to ask your spine surgeon before surgery will help you feel better prepared and more confident as you prepare for your procedure.
This list of 40 questions to ask your spine surgeon before surgery will help you feel better prepared and more confident as you prepare for your procedure.

Here are 5 exercises to stretch and strengthen the soft tissues in your upper and middle back, also known as the thoracic spine.
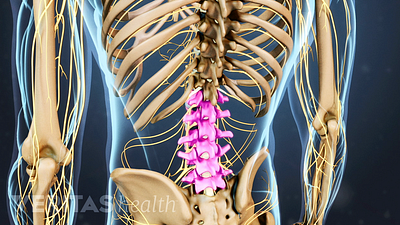
Understanding the anatomy of your lower spine will help you communicate more effectively with your back care providers.
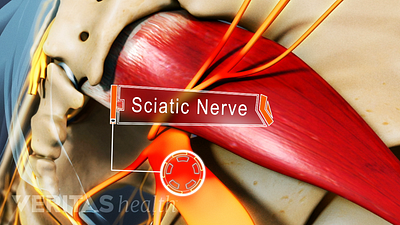
Use these 6 helpful tips to communicate your sciatica symptoms more effectively during your visit to the doctor.
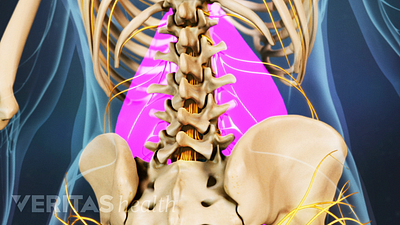
Learn about proven treatments that you can employ at home to reduce the pain from your pulled lower back muscle and also promote healing in the process.

When neck pain strikes, you may wonder if it's the result of a muscle strain or something more serious, like a problem in the cervical spine. Here are some clues to help you figure it out.
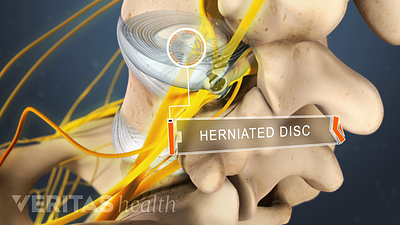
Home remedies that treat inflammation and reduce pressure on the spinal discs provide pain relief and facilitate healing from a herniated disc in the lower back.

Injury to certain important structures in your lower back may cause alarming symptoms that must be treated on an urgent basis. Read on to learn about 3 such red-flag symptoms.
Learn about 7 commonly overlooked tips that can help protect and stabilize your lower back.
There are rare sciatica-related symptoms that may indicate a severe injury to your spinal nerve roots and/or your spinal cord. Read on to learn about two such symptoms that require immediate medical attention.



