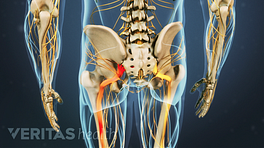
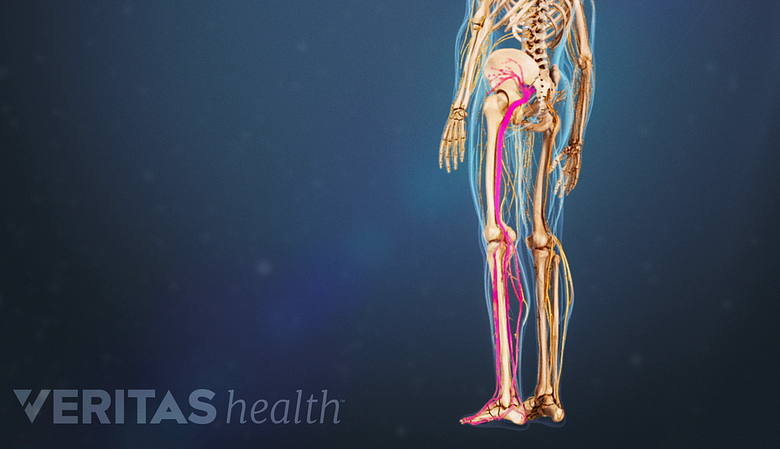
Sciatica is a term used to describe radiating pain that travels along the path of the sciatic nerve, running from your lower spine through the buttock and down the back of the leg. It flares when the sciatic nerve is irritated or pinched by any of a range of problems in your lower back.

Sciatica is nerve pain
There are a series of nerve roots that exit from your lower spine. When any of these nerve roots on either side of your lower spine becomes irritated or pinched, pain may radiate from the nerve root to the sciatic nerve. The pain may travel down the sciatic nerve – through the buttock and down the back of the leg and into your foot and/or toes. It typically occurs only on one side of the body.
See Types of Sciatic Nerve Pain
The pain is unique – often described as a shooting, searing pain that is felt deep in the buttock and radiates down the back of the leg. Numbness, tingling, or burning may also be felt along the nerve. Some people describe the nerve pain as electric-like. Conversely, sciatica symptoms may be experienced as more of a constant, dull pain.
Medical terms used for sciatica include lumbar radicular pain and lumbar radiculopathy.
Common lower back problems that cause sciatica
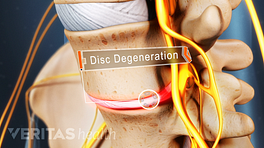
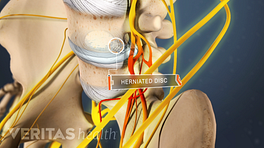
The most common cause of sciatica is a lumbar herniated disc 1 Kumar, M. Epidemiology, pathophysiology and symptomatic treatment of sciatica: A review. Int. J. Pharm. Bio. Arch. 2011, 2(4):1050-61. . Other common causes may include lumbar spinal stenosis, facet joint osteoarthritis, lumbar degenerative disc disease, or spondylolisthesis.
Read more about Sciatica Causes
The term sciatica is often misused, and people may be tempted to self-diagnose and self-treat the wrong cause of their sciatica. Knowing the underlying cause of your sciatica symptoms is important in order to get the right treatment.
In This Blog Series:
- Is My Pain Sciatica or Something Else?
- 4 Commonly Overlooked Sciatica Remedies
- Is Surgery the Quickest Path to Sciatica Relief?
Some conditions mimic sciatica
A number of conditions can mimic the radiating pain, numbness, and tingling of sciatica. Learn more: Leg Pain and Numbness: What Might These Symptoms Mean?
Many people refer to any type of leg pain as sciatica, but in fact, there are many causes of leg pain that are not medically classified as sciatica and need to be treated differently.
Examples of problems that are not sciatica but can cause similar symptoms include:
- Joint problems in the spine. Pain may be referred from the spinal joints down into the leg. This problem is technically not sciatica, and the treatment for it is different. For example, joint degeneration from spinal arthritis may cause pain that has sciatica-type symptoms.
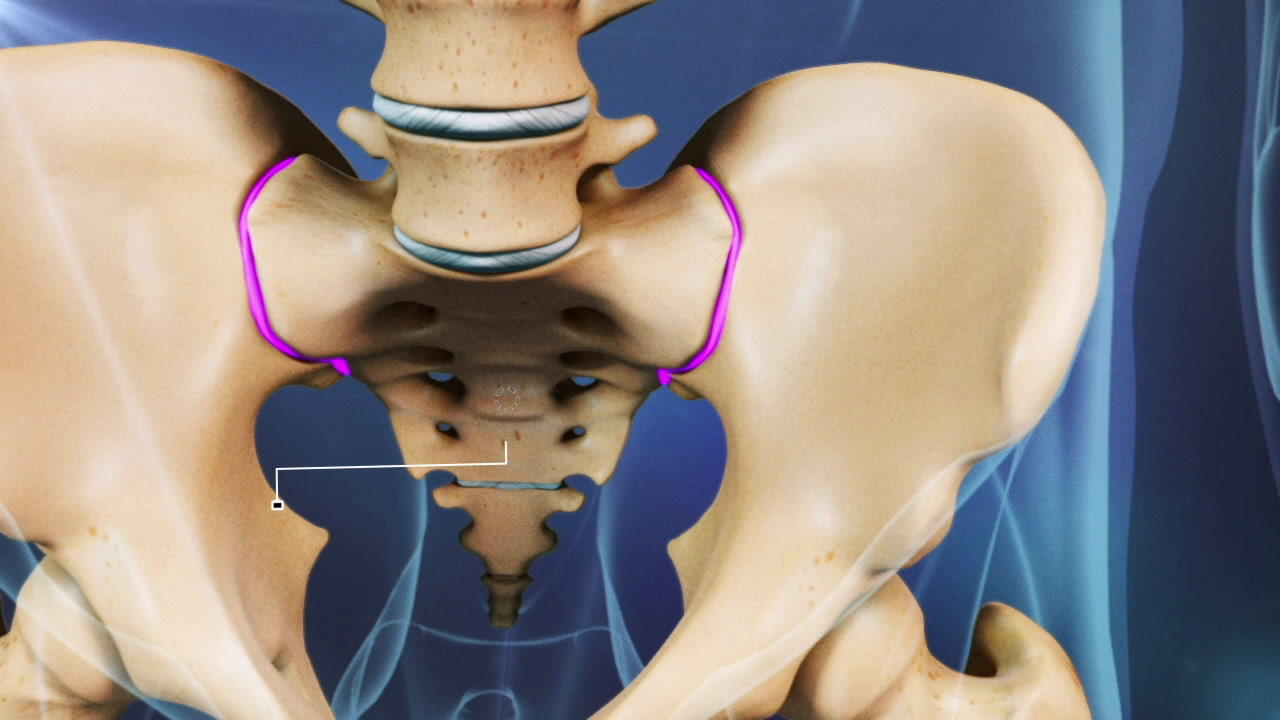
- Sacroiliac joint dysfunction. Too much or too little motion in the sacroiliac joints can cause pain that radiates down your leg and feels like sciatica. Treatment for sacroiliac joint dysfunction is usually non-surgical and focuses on restoring normal motion in the joint. Sacroiliac joint fusion is available if the pain is severe and debilitating.
- Piriformis syndrome also causes symptoms similar to sciatica. It occurs when the piriformis muscle in the buttocks irritates the sciatic nerve, which can cause pain to radiate along the path of the nerve into your leg. This type of pain is technically not sciatica, because the nerve irritation does not originate in the lower back. Treatment for piriformis syndrome usually includes anti-inflammatory medication and specific physical therapy.

Self-diagnosis of sciatica is not a good idea
As many underlying conditions can cause sciatic pain, it is important to consult a doctor for a clinical diagnosis. While rare, sciatica-like pain may be caused by medical conditions that need immediate treatment, such as:
While the vast majority of causes of sciatica symptoms are not serious, it is always advisable to see a doctor for any troubling symptoms.
If you feel symptoms of pain in your buttocks or leg, or numbness, tingling, or other neurological symptoms in your leg, it is important to see a doctor for clinical diagnosis that identifies the cause of your symptoms.
As you can see by reading the peer-reviewed articles on this site, treatment can be quite different depending on the underlying cause of your symptoms. For example:
- A lumbar herniated disc and lumbar stenosis can cause similar sciatica symptoms; however, physical therapy for each condition can be different—while bending forward at the waist may be comfortable if you have spinal stenosis, it can cause increased pain if you have a lumbar herniated disc.
- If spondylolisthesis is causing your sciatica, a doctor may advise fusion surgery to align and stabilize the affected segment before doing any sort of exercise.
Commit to a progressive exercise program for long-term pain relief
When your doctor gives you the go ahead, make sure to make a focused effort to follow through with a controlled and progressive exercise program. Without it, your symptoms are likely to return and get worse over time.
See Physical Therapy and Exercise for Sciatica
There are many options to help provide enough pain relief for you to engage in exercise and physical therapy, such as use of ice and heat, pain medications, and possibly an epidural steroid injection. Physical therapists and spine specialists can tailor a pain relief treatment to make exercise tolerable.
Read more about Sciatica Treatment
Learn more:
- 1 Kumar, M. Epidemiology, pathophysiology and symptomatic treatment of sciatica: A review. Int. J. Pharm. Bio. Arch. 2011, 2(4):1050-61.