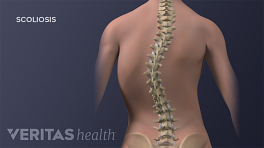
The optimal time to treat a progressing idiopathic scoliosis curve is typically before the adolescent growth spurt when the curve might rapidly worsen. Current medical literature tends to favor wearing a rigid back brace during this crucial period to lower the chance of developing a severe spinal deformity.
In This Article:
- Bracing Treatment for Idiopathic Scoliosis
- Types of Scoliosis Braces
- Controversy Over Whether Bracing Works
- Idiopathic Scoliosis Video
When to Think About Bracing
Bracing is prescribed based on the Cobb angle and its progression over time.
Scoliosis is considered any lateral (sideways) curvature of the spine that is at least 10 degrees as measured by the Cobb angle, which is found by examining an x-ray of the back. When a Cobb angle is above 10 degrees but less than 25 degrees, typically the recommended course of action is observation. This means every 4 to 6 months the doctor takes another x-ray to see if the curve is progressing or not.
See Spinal Anatomy and Back Pain
Bracing will often be prescribed if either of the following two conditions are met:
- Cobb angle has reached at least 25 degrees and the adolescent still has significant growth left until skeletal maturity
- Cobb angle is less than 25 degrees but has rapidly progressed at least 5 degrees at the 4- to 6-month follow-up appointment
See Cobb Angle Measurement and Treatment Guidelines
If the adolescent with scoliosis is at or near full skeletal maturity, bracing is unlikely to be prescribed because it would no longer be effective.
See Cobb Angle and Skeletal Maturity
The Goal of Bracing
A scoliosis curve usually does not improve without surgery. However, studies have shown that wearing a back brace as prescribed can often prevent the progression of scoliosis. As such, wearing a brace can be an effective way to keep a scoliosis curve’s Cobb angle relatively small and manageable.
A scoliosis curve that is 50 degrees by the time an adolescent reaches skeletal maturity (about age 14 or 15 for girls and 16 or 17 for boys) will continue to progress throughout adulthood.
These types of curves are likely to become a severe deformity that requires surgery. Therefore, the goal of bracing is to avoid a major surgery by either stopping curve progression altogether or at least preventing it from reaching 40 or 50 degrees at the time of skeletal maturity.
How Bracing Works
Bracing treatment aims to apply corrective forces on the spine to release load on the concave (inner) part of the curve and increase load on the convex (outer) part of the curve.
The idea is that a bone experiencing compression will grow less and a bone experiencing distraction (less or no compression) may grow more. Bracing tries to slow down the scoliosis curve’s bone growth on the side that needs to be slowed, and speed up growth on the side that needs to speed up.
While bracing will not typically reverse or correct with bracing, it can slow or reduce any progression of the curve until the child reaches skeletal maturity. After this point, the bones are unlikely to so the curve is unlikely to progress (provided it is less than 40 degrees).
The exact mechanisms of bracing are still being studied. However, literature indicates that the brace needs to be rigid (hard) in order to apply strong and consistent pressure on the scoliosis curve to have an effect. Therefore, rigid braces are the focus of this article.
See Treatment for Degenerative Scoliosis
Improvements in Bracing
The first cervico-thoraco-lumbo-sacral orthosis (CTLSO), called the Milwaukee brace, was invented in the 1940s. While this brace was innovative at the time, it was bulky and included metal bars up to the neck. The Milwaukee brace was uncomfortable to wear and also brought unwanted attention (especially for teenagers trying to fit in with peers).
Few patients benefited from this brace because few were willing or able to wear it anywhere near the prescribed 23 hours per day.
See When a Teen with Scoliosis Won’t Wear a Back Brace
By the 1970s and 80s, new brace options became available. Two significant breakthroughs included:
- Thoraco-lumbo-sacral orthosis (TLSO). The relatively snug-fitting TLSO braces start beneath the shoulders and are considered low-profile braces because they can be discreetly worn beneath loose-fitting clothes. Compared to the Milwaukee brace or CTLSO, the TLSO has no metal bars or cervical (neck) component.
- Nighttime brace. This type of brace puts greater forces on the spine while worn during sleep to make up for not wearing the brace during daytime hours. Since the nighttime brace is only worn while laying down (sleeping), it can apply greater force on the spine by not needing a counterbalance to keep the head aligned over the hips for walking or other movements.
TLSO and nighttime braces are discussed in more detail on the next page.