An autograft is a portion of bone transplanted from one part of a patient’s body to another. 1 D'Souza M, Macdonald NA, Gendreau JL, Duddleston PJ, Feng AY, Ho AL. Graft Materials and Biologics for Spinal Interbody Fusion. Biomedicines. 2019 Sep 26;7(4):75. doi: 10.3390/biomedicines7040075. PMID: 31561556; PMCID: PMC6966429. Autografts are also referred to as autologous bone or autogenous bone grafts.
Autografts offer numerous potential advantages and are considered the benchmark for spinal fusion procedures. 1 D'Souza M, Macdonald NA, Gendreau JL, Duddleston PJ, Feng AY, Ho AL. Graft Materials and Biologics for Spinal Interbody Fusion. Biomedicines. 2019 Sep 26;7(4):75. doi: 10.3390/biomedicines7040075. PMID: 31561556; PMCID: PMC6966429.
In This Article:
- Bone Graft for Spine Fusion
- Autograft: The Patient's Own Bone
- Allograft: Bone Graft from a Donor
- Bone Graft Substitutes
Harvesting Autografts
Bone from the patient's hip is harvested and transplanted in an autograft surgery.
Procuring autografts involves a separate surgical procedure, which includes removing bone from a different part of the patient’s body and placing it in the area of the spine to be fused. This surgical process is called "harvesting" the bone graft.
In a spinal fusion surgery, the harvesting procedure is usually done through the same incision in posterior fusions (fusions approached from the back of the body) and through a separate incision in anterior fusions (fusions approached from the front of the body).
In most cases, the patient’s hip bone (iliac crest) is harvested and transplanted in the segment of the spine where fusion is intended. 1 D'Souza M, Macdonald NA, Gendreau JL, Duddleston PJ, Feng AY, Ho AL. Graft Materials and Biologics for Spinal Interbody Fusion. Biomedicines. 2019 Sep 26;7(4):75. doi: 10.3390/biomedicines7040075. PMID: 31561556; PMCID: PMC6966429.
Other potential locations for harvesting autografts for spinal fusions include the thigh, leg, rib, spinal, or hand bones. However, to minimize the need for surgery in two separate areas, the hip is frequently chosen because of its proximity to the spine. 1 D'Souza M, Macdonald NA, Gendreau JL, Duddleston PJ, Feng AY, Ho AL. Graft Materials and Biologics for Spinal Interbody Fusion. Biomedicines. 2019 Sep 26;7(4):75. doi: 10.3390/biomedicines7040075. PMID: 31561556; PMCID: PMC6966429.
Types of Autografts
Based on the type of bone that is harvested, autografts can be of 2 types:
Cortical autografts
Cortical bone has high density and low porosity. When this bone is used as a grafting material, its robust and compact nature furnishes stability to the spinal segment during the initial phases of bone repair and reconstruction. 1 D'Souza M, Macdonald NA, Gendreau JL, Duddleston PJ, Feng AY, Ho AL. Graft Materials and Biologics for Spinal Interbody Fusion. Biomedicines. 2019 Sep 26;7(4):75. doi: 10.3390/biomedicines7040075. PMID: 31561556; PMCID: PMC6966429.
Due to the dense nature of this bone, the process of bone resorption and deposition is comparatively slow when it’s used as a graft. 1 D'Souza M, Macdonald NA, Gendreau JL, Duddleston PJ, Feng AY, Ho AL. Graft Materials and Biologics for Spinal Interbody Fusion. Biomedicines. 2019 Sep 26;7(4):75. doi: 10.3390/biomedicines7040075. PMID: 31561556; PMCID: PMC6966429.
Cancellous autografts
Cancellous bone, on the other hand, features higher porosity and lower density. When utilizing cancellous bone for grafting purposes, the large surface area of this porous tissue expedites the processes of bone resorption and deposition more effectively and swiftly. 1 D'Souza M, Macdonald NA, Gendreau JL, Duddleston PJ, Feng AY, Ho AL. Graft Materials and Biologics for Spinal Interbody Fusion. Biomedicines. 2019 Sep 26;7(4):75. doi: 10.3390/biomedicines7040075. PMID: 31561556; PMCID: PMC6966429.
The initial mechanical strength of this graft is limited, but it progressively ameliorates as new bone formation takes place. 1 D'Souza M, Macdonald NA, Gendreau JL, Duddleston PJ, Feng AY, Ho AL. Graft Materials and Biologics for Spinal Interbody Fusion. Biomedicines. 2019 Sep 26;7(4):75. doi: 10.3390/biomedicines7040075. PMID: 31561556; PMCID: PMC6966429.
The quality of individual grafts differs based on the patient’s age, bone health, and metabolic activity. 1 D'Souza M, Macdonald NA, Gendreau JL, Duddleston PJ, Feng AY, Ho AL. Graft Materials and Biologics for Spinal Interbody Fusion. Biomedicines. 2019 Sep 26;7(4):75. doi: 10.3390/biomedicines7040075. PMID: 31561556; PMCID: PMC6966429.
Potential Benefits of Autografts
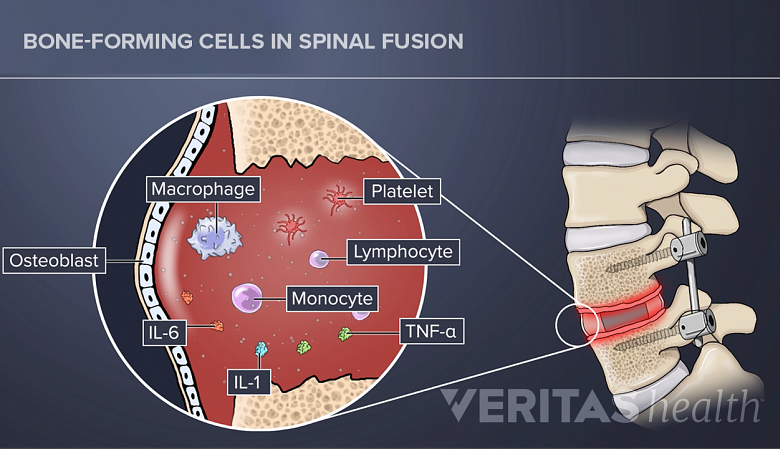
Autograft contains live bone-forming cells such as osteoblasts and growth factors.
Autografts contain several essential properties that make them more suitable for bone healing and fusion when compared to other graft types 2 Lombardo JA, Russell N, He J, Larson MJ, Walsh WR, Mundis GM Jr, Vizesi F. Autograft Cellular Contribution to Spinal Fusion and Effects of Intraoperative Storage Conditions. Spine (Phila Pa 1976). 2023 Aug 15;48(16):1181-1189. doi: 10.1097/BRS.0000000000004688. Epub 2023 Apr 20. PMID: 37078877; PMCID: PMC10368216. :
- They possess a ready-to-use cortical or cancellous bone scaffold, which provides the base for new bone to grow on.
- They contain live bone-forming cells, such as osteoblasts, osteoclasts, osteocytes, and osteogenic precursor cells. These are called adherent cells and play a significant role in the fusion process.
- They contain matrices and growth factors that boost bone growth through chemical processes.
Since autografts are the patient's own bone tissue, the likelihood of the body rejecting the graft as a foreign entity is low. 3 Baldwin P, Li DJ, Auston DA, Mir HS, Yoon RS, Koval KJ. Autograft, Allograft, and Bone Graft Substitutes: Clinical Evidence and Indications for Use in the Setting of Orthopaedic Trauma Surgery. J Orthop Trauma. 2019;33(4):203-213. doi:10.1097/BOT.0000000000001420 Additionally, the risk of disease transmission (vs cadaver bone) is less.
Potential Risks and Drawbacks of Autografts
Autografts present certain potential risks that warrant careful consideration. Around 10% to 39% of patients experience varying degrees of risks with autograft harvesting.
- Ongoing chronic pain at the graft harvest site is a common side effect of autograft harvesting and is seen in over 25% of patients who undergo spinal fusion surgery. 4 Carlisle ER, Fischgrund JS. Bone graft and fusion enhancement. In: Surgical Management of Spinal Deformities. Elsevier; 2009:433-448.
- Major complications occur in about 0.7% to 25% of cases and include excessive bleeding, herniation, serious infection, scarring, hematoma (pooling of blood) formation, injury to nerves or blood vessels, and pelvic fracture. 4 Carlisle ER, Fischgrund JS. Bone graft and fusion enhancement. In: Surgical Management of Spinal Deformities. Elsevier; 2009:433-448.
- Less severe risks include superficial infections, transient sensory impairment, and milder pain that resolves over time. 4 Carlisle ER, Fischgrund JS. Bone graft and fusion enhancement. In: Surgical Management of Spinal Deformities. Elsevier; 2009:433-448.
- A higher risk of sacroiliac joint dysfunction or dislocation is associated with surgeries approached from the back, such as PLIF. 4 Carlisle ER, Fischgrund JS. Bone graft and fusion enhancement. In: Surgical Management of Spinal Deformities. Elsevier; 2009:433-448.
- A higher risk of infection is associated with surgeries approached from the front, such as ALIF. 4 Carlisle ER, Fischgrund JS. Bone graft and fusion enhancement. In: Surgical Management of Spinal Deformities. Elsevier; 2009:433-448.
Autografts also have limited availability, particularly in cases where the patient has insufficient healthy bone to spare for grafting. In some cases, the quality of autografts may be compromised if the patient's age and overall health are unfavorable, potentially affecting the graft's effectiveness in promoting fusion.
These potential disadvantages emphasize the importance of thorough presurgical assessment, patient education, and close postsurgical monitoring to mitigate and manage any complications that may arise.
Avoiding Autograft Risks
The most commonly occurring risk of harvesting an autograft is ongoing pain at the bone graft site. 5 Morris MT, Tarpada SP, Cho W. Bone graft materials for posterolateral fusion made simple: a systematic review [published correction appears in Eur Spine J. 2021 Aug;30(8):2410-2411]. Eur Spine J. 2018;27(8):1856-1867. doi:10.1007/s00586-018-5511-6 This pain develops as a result of injury to the muscle or small sensory nerves near the pelvis (iliac crest), from where the bone graft is usually harvested. Both of these pitfalls may be avoided by optimizing the harvest process:
- In a PLIF and posterolateral gutter spine fusion, the bone harvest procedure can be done through the same incision as the spinal fusion surgery. 6 France JC, Schuster JM, Moran K, Dettori JR. Iliac Crest Bone Graft in Lumbar Fusion: The Effectiveness and Safety Compared with Local Bone Graft, and Graft Site Morbidity Comparing a Single-Incision Midline Approach with a Two-Incision Traditional Approach. Global Spine J. 2015 Jun;5(3):195-206. doi: 10.1055/s-0035-1552985. PMID: 26131386; PMCID: PMC4472292. This method avoids damage to nerves or blood vessels, and only muscles at the top portion of the iliac crest need to be stripped. The use of this surgical technique also minimizes the blood loss and post-surgical pain associated with bone graft harvesting.
- Bone harvested for ALIF needs to be approached through a separate incision (1-2 inches long) over the pelvis. With careful surgical technique, however, only the very top portion of the iliac crest needs to be removed to harvest the bone graft. Care is needed to avoid the lateral femoral cutaneous nerve in this area, as damage to this nerve can result in chronic pain and numbness in the front of the thigh.
Additionally, augmenting a small portion of harvested tissue with other graft types, such as allografts and bone graft substitutes, helps reduce the overall amount of bone harvest. 5 Morris MT, Tarpada SP, Cho W. Bone graft materials for posterolateral fusion made simple: a systematic review [published correction appears in Eur Spine J. 2021 Aug;30(8):2410-2411]. Eur Spine J. 2018;27(8):1856-1867. doi:10.1007/s00586-018-5511-6
Bone Marrow Aspirates: Preserving the Benefits and Overcoming the Drawbacks of Autografts
Considering the limitations and potential complications associated with harvesting autografts, researchers have turned to bone marrow aspirates as an alternative to using hip bone tissue for spinal fusion.
Bone marrow aspirate can be directly sourced from the patient’s hip bone and contains the essential cells that are needed to initiate and continue bone healing and remodeling. The marrow tissue is extracted using large bore needles and causes minimal damage to the donor site.
- 1 D'Souza M, Macdonald NA, Gendreau JL, Duddleston PJ, Feng AY, Ho AL. Graft Materials and Biologics for Spinal Interbody Fusion. Biomedicines. 2019 Sep 26;7(4):75. doi: 10.3390/biomedicines7040075. PMID: 31561556; PMCID: PMC6966429.
- 2 Lombardo JA, Russell N, He J, Larson MJ, Walsh WR, Mundis GM Jr, Vizesi F. Autograft Cellular Contribution to Spinal Fusion and Effects of Intraoperative Storage Conditions. Spine (Phila Pa 1976). 2023 Aug 15;48(16):1181-1189. doi: 10.1097/BRS.0000000000004688. Epub 2023 Apr 20. PMID: 37078877; PMCID: PMC10368216.
- 3 Baldwin P, Li DJ, Auston DA, Mir HS, Yoon RS, Koval KJ. Autograft, Allograft, and Bone Graft Substitutes: Clinical Evidence and Indications for Use in the Setting of Orthopaedic Trauma Surgery. J Orthop Trauma. 2019;33(4):203-213. doi:10.1097/BOT.0000000000001420
- 4 Carlisle ER, Fischgrund JS. Bone graft and fusion enhancement. In: Surgical Management of Spinal Deformities. Elsevier; 2009:433-448.
- 5 Morris MT, Tarpada SP, Cho W. Bone graft materials for posterolateral fusion made simple: a systematic review [published correction appears in Eur Spine J. 2021 Aug;30(8):2410-2411]. Eur Spine J. 2018;27(8):1856-1867. doi:10.1007/s00586-018-5511-6
- 6 France JC, Schuster JM, Moran K, Dettori JR. Iliac Crest Bone Graft in Lumbar Fusion: The Effectiveness and Safety Compared with Local Bone Graft, and Graft Site Morbidity Comparing a Single-Incision Midline Approach with a Two-Incision Traditional Approach. Global Spine J. 2015 Jun;5(3):195-206. doi: 10.1055/s-0035-1552985. PMID: 26131386; PMCID: PMC4472292.