Synthetic bone graft substitutes are man-made alternatives to real bone tissue. They mimic the structure and biomechanical properties of real bone. They allow for bone growth on their surface, and then they are resorbed by the body, with the patient’s own bone remaining in place.
However, these products do not have all the properties necessary to stimulate spinal fusion when used alone. They are usually used in combination with the patient’s own bone to augment the amount of bone graft available.
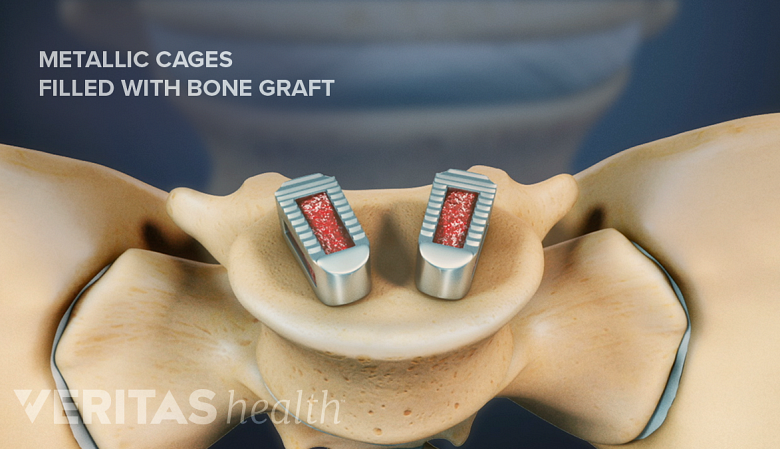
Synthetic bone graft substitutes mimic real bone and promote bone growth.
In This Article:
- Bone Graft for Spine Fusion
- Autograft: The Patient's Own Bone
- Allograft: Bone Graft from a Donor
- Bone Graft Substitutes
Bone tissue engineering is an emerging technology in the field of regenerative medicine that aims to create functional bone graft substitutes. 1 Gao C, Deng Y, Feng P, Mao Z, Li P, Yang B, Deng J, Cao Y, Shuai C, Peng S. Current progress in bioactive ceramic scaffolds for bone repair and regeneration. Int J Mol Sci. 2014 Mar 18;15(3):4714-32. doi: 10.3390/ijms15034714. PMID: 24646912; PMCID: PMC3975421.
These substitutes consist of scaffold materials that provide structural support while encouraging cell attachment and growth. The scaffold can be augmented with stem cells, growth factors, and biocompatible materials to contribute to the formation of new bone tissue, tailored to the needs of individual patients. 1 Gao C, Deng Y, Feng P, Mao Z, Li P, Yang B, Deng J, Cao Y, Shuai C, Peng S. Current progress in bioactive ceramic scaffolds for bone repair and regeneration. Int J Mol Sci. 2014 Mar 18;15(3):4714-32. doi: 10.3390/ijms15034714. PMID: 24646912; PMCID: PMC3975421.
Ceramics in Spinal Fusion
Bioactive ceramics possess a unique ability to bond with living tissues and promote regenerative processes. 1 Gao C, Deng Y, Feng P, Mao Z, Li P, Yang B, Deng J, Cao Y, Shuai C, Peng S. Current progress in bioactive ceramic scaffolds for bone repair and regeneration. Int J Mol Sci. 2014 Mar 18;15(3):4714-32. doi: 10.3390/ijms15034714. PMID: 24646912; PMCID: PMC3975421. Examples of commonly used ceramics in spinal fusion include 2 Ortega B, Gardner C, Roberts S, Chung A, Wang JC, Buser Z. Ceramic Biologics for Bony Fusion-a Journey from First to Third Generations. Curr Rev Musculoskelet Med. 2020 Aug;13(4):530-536. doi: 10.1007/s12178-020-09651-x. PMID: 32562147; PMCID: PMC7340712. :
- Hydroxyapatite. Hydroxyapatite is a naturally occurring calcium salt in the human bone and the most commonly used ceramic bone graft substitute or bone graft extender.
- This compound provides the scaffolding for the bone graft but does not contain the cells or growth factors to initiate bone regeneration and fusion.
- For this reason, hydroxyapatite is augmented with bone-forming cells and growth factors before it is used as a graft.
- Hydroxyapatite is inert, easy to sterilize, and readily available for use.
- Beta-tricalcium phosphate (β-TCP). β-TCP contains 39% calcium and 20% phosphate and shares a similar structure with normal bone. It is used as a bone graft substitute and bone graft extender.
- Like hydroxyapatite, β-TCP provides scaffolding and can be augmented with cells and growth factors.
- β-TCP is a porous ceramic and resorbs faster than hydroxyapatite, which may be a disadvantage when used in strength-bearing areas of the spine.
- Calcium sulfate. Calcium sulfate has a crystalline structure and mimics cancellous bone (bone that is more porous and less dense).
- Calcium sulfate resorbs quickly and is generally used along with another graft material, such as allograft.
- It can be augmented with cells and growth factors to improve bone remodeling and fusion.
- Calcium sulfate has a comparatively lower cost, making it a popular graft option in some surgical procedures.
The most common use of ceramics in spinal fusion is as a bone graft extender in posterolateral gutter fusions. 2 Ortega B, Gardner C, Roberts S, Chung A, Wang JC, Buser Z. Ceramic Biologics for Bony Fusion-a Journey from First to Third Generations. Curr Rev Musculoskelet Med. 2020 Aug;13(4):530-536. doi: 10.1007/s12178-020-09651-x. PMID: 32562147; PMCID: PMC7340712.
Bone Morphogenetic Protein (BMP)
Bone morphogenetic protein (BMP) refers to over 20 different types of specialized proteins and growth factors that stimulate bone growth naturally in the human body. 3 D'Souza M, Macdonald NA, Gendreau JL, Duddleston PJ, Feng AY, Ho AL. Graft Materials and Biologics for Spinal Interbody Fusion. Biomedicines. 2019 Sep 26;7(4):75. doi: 10.3390/biomedicines7040075. PMID: 31561556; PMCID: PMC6966429.
These proteins that exist in the body can be produced, concentrated, and placed in the area of the spine for a spinal fusion to take place. More importantly, they can create a fusion without the need for any use of the patient’s own bone. 3 D'Souza M, Macdonald NA, Gendreau JL, Duddleston PJ, Feng AY, Ho AL. Graft Materials and Biologics for Spinal Interbody Fusion. Biomedicines. 2019 Sep 26;7(4):75. doi: 10.3390/biomedicines7040075. PMID: 31561556; PMCID: PMC6966429.
BMP is a popular choice among spine surgeons because of consistent results and low complication rates for posterolateral gutter fusion and anterior lumbar fusion (such as anterior lumbar interbody fusion or ALIF) techniques. 4 Reisener MJ, Pumberger M, Shue J, Girardi FP, Hughes AP. Trends in lumbar spinal fusion-a literature review. J Spine Surg. 2020;6(4):752-761. doi:10.21037/jss-20-492 , 5 Oliveira OR, Martins SP, Lima WG, Gomes MM. The use of bone morphogenetic proteins (BMP) and pseudarthrosis, a literature review. Rev Bras Ortop. 2016;52(2):124-140. Published 2016 Jun 22. doi:10.1016/j.rboe.2016.03.005 In posterolateral lumbar fusions, BMP is often supplemented with cancellous allograft. 6 Guerado E, Cervan AM, Bertrand ML, Benitez-Parejo N. Allograft plus OP-1 enhances ossification in posterolateral lumbar fusion: A seven year follow-up. Injury. 2016;47 Suppl 3:S78-S82. doi:10.1016/S0020-1383(16)30611-8
Types of bone morphogenetic proteins (BMP)
While there are several different BMPs naturally found in the body, research has focused on BMP-2, BMP-4, and BMP-7. The primary goals of using BMP in spinal fusions are 3 D'Souza M, Macdonald NA, Gendreau JL, Duddleston PJ, Feng AY, Ho AL. Graft Materials and Biologics for Spinal Interbody Fusion. Biomedicines. 2019 Sep 26;7(4):75. doi: 10.3390/biomedicines7040075. PMID: 31561556; PMCID: PMC6966429. :
- To create a spinal fusion as well as the patient’s own bone.
- To eliminate the need for harvesting the patient's bone – avoiding the potential side effects and complications of the bone harvesting procedure.
BMPs are used in a synthetic carrier medium (such as ceramics) or they may be added to an autograft or allograft material. 3 D'Souza M, Macdonald NA, Gendreau JL, Duddleston PJ, Feng AY, Ho AL. Graft Materials and Biologics for Spinal Interbody Fusion. Biomedicines. 2019 Sep 26;7(4):75. doi: 10.3390/biomedicines7040075. PMID: 31561556; PMCID: PMC6966429.
Risks, complications, and considerations with bone morphogenetic proteins
In 2002, BMP was approved by the US Food and Drug Administration (FDA) for use in ALIF surgeries, but the material quickly gained popularity and was used off-label in other fusion procedures, such as cervical fusions. 7 Guzman JZ, Merrill RK, Kim JS, et al. Bone morphogenetic protein use in spine surgery in the United States: how have we responded to the warnings?. Spine J. 2017;17(9):1247-1254. doi:10.1016/j.spinee.2017.04.030
The use of BMP in posterior lumbar interbody fusion (PLIF) and transforaminal lumbar interbody fusion (TLIF) has been associated with the development of sterile abscess (collection of fluid as a result of inflammation) in the epidural space and should be avoided. 8 James AW, LaChaud G, Shen J, et al. A Review of the Clinical Side Effects of Bone Morphogenetic Protein-2. Tissue Eng Part B Rev. 2016;22(4):284-297. doi:10.1089/ten.TEB.2015.0357
Several complications and risks have been noted with BMP use in cervical fusion surgeries, and in 2008, the FDA released an advisory warning about complications reported with the use of BMP-2 in ACDF surgeries. Specifically, the following risks were noted 7 Guzman JZ, Merrill RK, Kim JS, et al. Bone morphogenetic protein use in spine surgery in the United States: how have we responded to the warnings?. Spine J. 2017;17(9):1247-1254. doi:10.1016/j.spinee.2017.04.030 :
- Swelling of neck and throat tissue
- Compression of the airway and/or neurological structures in the neck
Some patients also reported difficulty swallowing, breathing, and/or speaking. 7 Guzman JZ, Merrill RK, Kim JS, et al. Bone morphogenetic protein use in spine surgery in the United States: how have we responded to the warnings?. Spine J. 2017;17(9):1247-1254. doi:10.1016/j.spinee.2017.04.030 For these reasons, it is not recommended that BMP-2 be used for anterior cervical fusions as there are other effective options.
- 1 Gao C, Deng Y, Feng P, Mao Z, Li P, Yang B, Deng J, Cao Y, Shuai C, Peng S. Current progress in bioactive ceramic scaffolds for bone repair and regeneration. Int J Mol Sci. 2014 Mar 18;15(3):4714-32. doi: 10.3390/ijms15034714. PMID: 24646912; PMCID: PMC3975421.
- 2 Ortega B, Gardner C, Roberts S, Chung A, Wang JC, Buser Z. Ceramic Biologics for Bony Fusion-a Journey from First to Third Generations. Curr Rev Musculoskelet Med. 2020 Aug;13(4):530-536. doi: 10.1007/s12178-020-09651-x. PMID: 32562147; PMCID: PMC7340712.
- 3 D'Souza M, Macdonald NA, Gendreau JL, Duddleston PJ, Feng AY, Ho AL. Graft Materials and Biologics for Spinal Interbody Fusion. Biomedicines. 2019 Sep 26;7(4):75. doi: 10.3390/biomedicines7040075. PMID: 31561556; PMCID: PMC6966429.
- 4 Reisener MJ, Pumberger M, Shue J, Girardi FP, Hughes AP. Trends in lumbar spinal fusion-a literature review. J Spine Surg. 2020;6(4):752-761. doi:10.21037/jss-20-492
- 5 Oliveira OR, Martins SP, Lima WG, Gomes MM. The use of bone morphogenetic proteins (BMP) and pseudarthrosis, a literature review. Rev Bras Ortop. 2016;52(2):124-140. Published 2016 Jun 22. doi:10.1016/j.rboe.2016.03.005
- 6 Guerado E, Cervan AM, Bertrand ML, Benitez-Parejo N. Allograft plus OP-1 enhances ossification in posterolateral lumbar fusion: A seven year follow-up. Injury. 2016;47 Suppl 3:S78-S82. doi:10.1016/S0020-1383(16)30611-8
- 7 Guzman JZ, Merrill RK, Kim JS, et al. Bone morphogenetic protein use in spine surgery in the United States: how have we responded to the warnings?. Spine J. 2017;17(9):1247-1254. doi:10.1016/j.spinee.2017.04.030
- 8 James AW, LaChaud G, Shen J, et al. A Review of the Clinical Side Effects of Bone Morphogenetic Protein-2. Tissue Eng Part B Rev. 2016;22(4):284-297. doi:10.1089/ten.TEB.2015.0357