
The initial 6-week recuperation period after a spinal fusion focuses on getting back to feeling good. After this initial period, more advanced exercise should be added to strengthen the back structures and increase overall fitness.
See Spinal Fusion Surgery Recovery: 1 to 3 Months After
Patients can add more rigor and variety to their routines by using an exercise ball or resistance bands.
The exact timing of when a surgeon will recommend adding dynamic exercises is dependent on both the quality of stability achieved at surgery and the surgeon's own personal preference.
See more about Dynamic Stabilization Exercises
In This Article:
- Rehabilitation Following Lumbar Fusion
- Guide to Physical Therapy After Spinal Fusion
- Physical Therapy after Spinal Fusion: Weeks 6 to 9
- Physical Therapy after Spinal Fusion: Weeks 9 to 12
Guide to Dynamic Exercises after Spine Fusion: Weeks 6-12
Because these exercises allow for motion of the trunk, many times they incorporate use of an exercise ball into the program.
Mat Movement Examples
Mat movement exercise strengthens the core by engaging abdominal and back muscles.
Do these exercises on a yoga or gym mat. If you don’t have a mat, try doing them on a rug or carpet.
- Strengthen abdominal muscles with a diagonal curl: while lying on the floor with knees bent, curl the trunk by raising the head and one shoulder towards opposite hip a few inches.
- Extend the back by alternating limbs: while on hands and knees, raise one arm and opposite leg, then alternate.
Band Movement Examples
Stretchy elastic bands called resistance bands are commonly used for strength training and physical therapy. They are sold in sports equipment stores, big-box stores, and online.
- Stretch the back by using a resistance band wrapped around a stationary pole or column, and leaning back with straight arms.
- Strengthen the abdominals and oblique muscles by performing a diagonal pull with the band: with the band anchored low to the ground, and feet shoulder-width apart, grasp band and pull from lower right to left shoulder. Reverse sides.
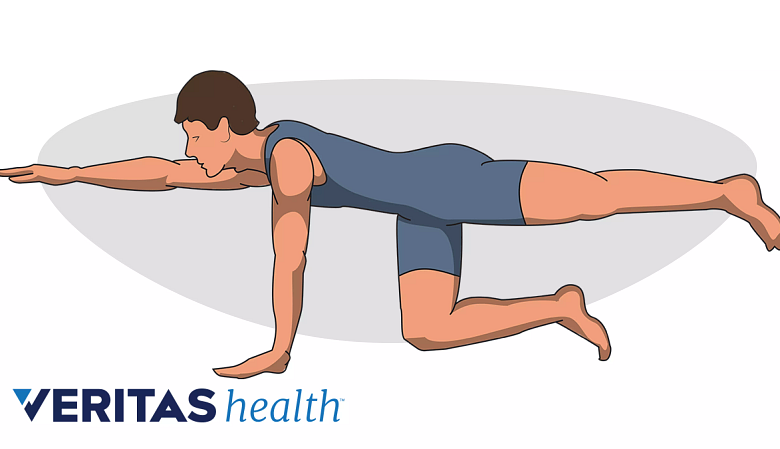
Exercise Ball Movement Examples
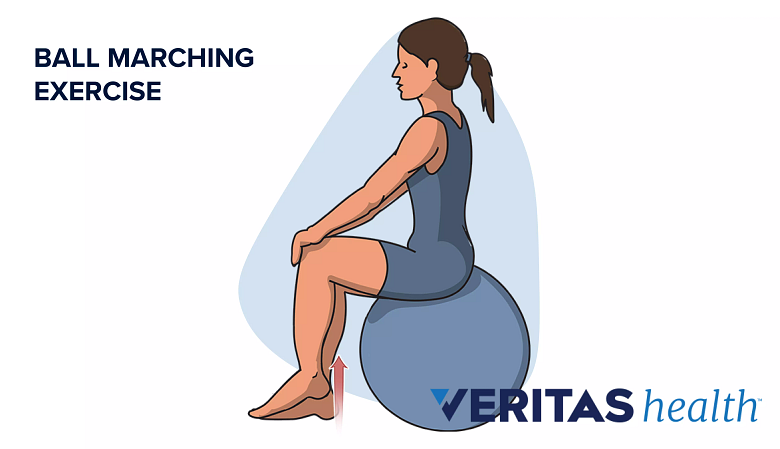
Ball marching exercises strengthen core muscles for lower back support.
When using an exercise ball, maximizing the range of motion is not as important as staying in control, which takes practice if a patient is not familiar with using an exercise ball. Don't worry about counting repetitions, but perform the exercise until fatigue is evident or control becomes difficult.
See more about Exercise Ball Therapy for Lower Back Pain Relief
A set should last 30 to 60 seconds (so about the length of a commercial break during a television show). One set a day is usually recommended.
- While lying with stomach on the exercise ball and arms/hands in front, walk forward on the ball until it rests under the thighs, then raise one leg at a time.
- With stomach on the exercise ball and knees on the ground, walk straight out on the hands, but don't let the trunk twist or dip down.
- Variation: With stomach on the exercise ball and feet on floor, raise head and chest from the forward bent position to a straight (but not hyper-extended) trunk.
- While lying on back with the exercise ball under the calves, raise buttocks, hips and lower back from the floor, keeping the stomach muscles tight.









