
Subscribe to our newsletter and get your FREE guide,
L5-S1 Symptoms Tracker.
The L5-S1 spinal motion segment, also called the lumbosacral joint, is the transition region between the lumbar spine and sacral spine in the lower back. In this region, the curvature of the spine changes from lumbar lordosis (forward curve) to sacral kyphosis (backward curve). L5-S1 helps transfer loads from the spine into the pelvis and legs.
The L5-S1 motion segment has distinctive anatomy and receives a higher degree of mechanical stress and loads compared to the segments above.1Cramer GD. The Lumbar Region. In: Clinical Anatomy of the Spine, Spinal Cord, and Ans. Elsevier; 2014:246-311. doi:10.1016/b978-0-323-07954-9.00007-4 These characteristics may make L5-S1 susceptible to traumatic injuries, degeneration, disc herniation, and/or nerve pain.
In This Article:
- All about L5-S1 (Lumbosacral Joint)
- L5-S1 Treatment
- Spinal Motion Segment: L5-S1 Animation
Anatomy of the L5-S1 Spinal Motion Segment
This motion segment typically includes the following structures:
L5 and S1 vertebrae

The L5-S1 segment spans two different portions of the spine, the lumbar and the sacral.
The L5 and S1 vertebrae have different features:
- L5 consists of a vertebral body in front and an arch in the back that has 3 bony protrusions: a prominent spinous process in the middle and two transverse processes on the sides. These protrusions serve as attachment points for ligaments.
- S1, also called the sacral base, is the upper and wider end of the triangular-shaped sacrum. S1 consists of a body on the top with wing-shaped bones on either side, called the alae. At the back, the S1 vertebra contains a long bony prominence called the median ridge. There are bony openings (foramina) on the right and left sides of this ridge.
- L5 and S1 are joined by the lumbosacral facet joints lined with articular cartilage.
L5-S1 intervertebral disc

The L5-S1 disc protects and structurally supports the vertebrae.
A disc made of a gel-like material (nucleus pulposus) surrounded by a thick fibrous ring (annulus fibrosus) is situated between the vertebral bodies of L5 and S1. This disc provides cushioning and shock-absorbing functions to protect the vertebrae during spinal movements.
Watch Lumbar Disc Anatomy Animation
L5 spinal nerve

Nerve roots branch out from the spinal cord at each spinal segment.
The L5 spinal nerve roots exit the spinal cord through small bony openings (intervertebral foramina) on the left and right sides of the spinal canal. These nerve roots join with other nerves to form bigger nerves that extend down the spine and travel down each leg.
- The L5 dermatome is an area of skin that receives sensations through the L5 spinal nerve and includes parts of the knee, leg, and foot.2Kayalioglu G. The Spinal Nerves. In: The Spinal Cord. Elsevier; 2009:37-56. doi:10.1016/b978-0-12-374247-6.50008-0
- The L5 myotome is a group of muscles controlled by the L5 spinal nerve and includes specific muscles in the pelvis and legs, which are responsible for leg and foot movements.2Kayalioglu G. The Spinal Nerves. In: The Spinal Cord. Elsevier; 2009:37-56. doi:10.1016/b978-0-12-374247-6.50008-0
The L5-S1 motion segment provides a bony enclosure for the cauda equina (nerves that continue down from the spinal cord) and other delicate structures.
advertisement
Common Problems at L5-S1
The L5-S1 situated at the bottom of the vertebral column is typically subject to excessive biomechanical stress, leading to more loads and an increased risk of injury. Common problems include:
Disc problems

The L5-S1 disc is vulnerable to herniation.
Lower back disc herniation typically occurs at the L5-S1 level.3Donnally III CJ, Butler AJ, Varacallo M. Lumbosacral Disc Injuries. [Updated 2019 Apr 11]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2019 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK448072/ A steeper inclination of this disc leads to a higher degree of shear stresses and increases the risk disc of injury and degeneration.
Facet joint pain

The facet joints can be damaged by inflammation or osteoarthritis.
The lumbosacral joint may develop wear-and-tear arthritis (osteoarthritis) over time due to its high load-bearing function.4Alexander CE, Varacallo M. Lumbosacral Facet Syndrome. [Updated 2019 Mar 23]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2019 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK441906/ Facet joint pain may also occur due to due to inflammatory conditions, such as rheumatoid arthritis or degenerative spondylolisthesis.5Perolat R, Kastler A, Nicot B, et al. Facet joint syndrome: from diagnosis to interventional management. Insights Imaging. 2018;9(5):773–789. doi:10.1007/s13244-018-0638-x
Spondylolysis
The L5 vertebra is susceptible to spondylolysis, which is the fracture of the pars interarticularis (a small segment of bone from the vertebral arch joining the facet joints) most commonly due to repetitive stress on the bone.1Cramer GD. The Lumbar Region. In: Clinical Anatomy of the Spine, Spinal Cord, and Ans. Elsevier; 2014:246-311. doi:10.1016/b978-0-323-07954-9.00007-4 It can occur on one or both sides. Frequently, the bone does not break, but becomes stressed and this condition is called a pars stress reaction.
Spondylolisthesis
If the pars of L5 fractures on both sides, the vertebra may slip over S1, a condition called spondylolisthesis. Most commonly, spondylolisthesis of L5 is caused by repetitive stress to the pars interarticularis and is most has commonly seen in children and adolescents.1Cramer GD. The Lumbar Region. In: Clinical Anatomy of the Spine, Spinal Cord, and Ans. Elsevier; 2014:246-311. doi:10.1016/b978-0-323-07954-9.00007-4 A pars fracture due to trauma is rather uncommon.
While rare, malignant tumors, such as sacral chondromas may occur in the L5-S1 level.6Pillai S, Govender S. Sacral chordoma : A review of literature. Journal of Orthopaedics. 2018;15(2):679-684. doi:10.1016/j.jor.2018.04.001 This level is also subject to other problems arising from developmental variations in the shape of S1, a fusion of L5 with S1, and the presence of extra facet joints between L5-S1.
Watch Isthmic Spondylolisthesis Video
Common Symptoms and Signs Stemming from L5-S1
Issues in the L5-S1 segment can cause pain throughout the lower body.
Vertebral and disc pain from L5-S1 may occur suddenly following an injury or gradually develop over a period of time. Typically, a dull ache or sharp pain may be felt in the lower back. Discogenic pain is typically worsened by prolonged sitting, standing in one place, and repetitive lifting and bending activities.
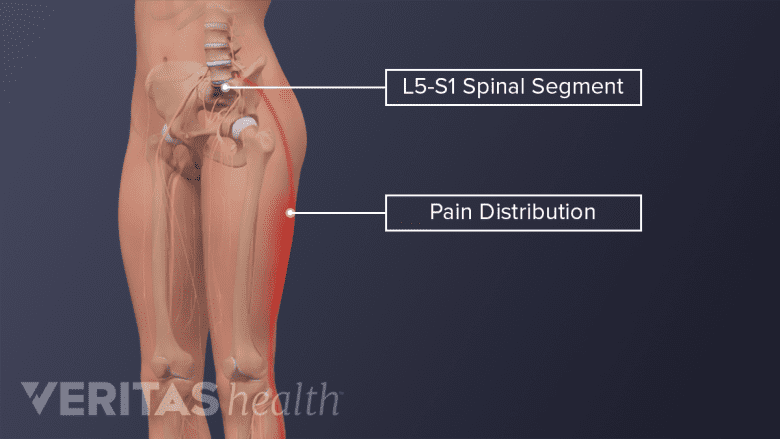
Compression or inflammation of the L5 and/or S1 spinal nerve root may cause radiculopathy symptoms or sciatica, characterized by:
- Pain, generally felt as a sharp, shooting, and/or searing feeling in the buttock, thigh, leg, foot, and/or toes
- Numbness in the foot and/or toes
- Weakness in the leg and/or foot muscles and an inability to lift the foot off the floor (foot drop)
It is also possible for a stabbing pain or ache to be isolated to any of these (dermatomal) areas. While these symptoms typically affect one leg at a time, sometimes, both legs may be affected together.
advertisement
Cauda equina syndrome may occur at L5-S1 due to an injury to the cauda equina nerves that descend from the spinal cord. This syndrome is a medical emergency and typically causes severe pain, weakness, numbness, and/or tingling in the groin, genital region, and/or both legs. There may also be loss of bowel and/or bladder control. The condition must be treated on an urgent basis to preserve leg function and restore bowel and/or bladder function.
See Cauda Equina Syndrome Symptoms
Nonsurgical treatments are often tried first for symptoms that stem from L5-S1. In rare cases, surgery may be considered.
- 1 Cramer GD. The Lumbar Region. In: Clinical Anatomy of the Spine, Spinal Cord, and Ans. Elsevier; 2014:246-311. doi:10.1016/b978-0-323-07954-9.00007-4
- 2 Kayalioglu G. The Spinal Nerves. In: The Spinal Cord. Elsevier; 2009:37-56. doi:10.1016/b978-0-12-374247-6.50008-0
- 3 Donnally III CJ, Butler AJ, Varacallo M. Lumbosacral Disc Injuries. [Updated 2019 Apr 11]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2019 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK448072/
- 4 Alexander CE, Varacallo M. Lumbosacral Facet Syndrome. [Updated 2019 Mar 23]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2019 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK441906/
- 5 Perolat R, Kastler A, Nicot B, et al. Facet joint syndrome: from diagnosis to interventional management. Insights Imaging. 2018;9(5):773–789. doi:10.1007/s13244-018-0638-x
- 6 Pillai S, Govender S. Sacral chordoma : A review of literature. Journal of Orthopaedics. 2018;15(2):679-684. doi:10.1016/j.jor.2018.04.001

advertisement