
Subscribe to our newsletter and get your FREE guide,
Natural Back Pain Relief: 16 Choices for Lasting Comfort.
When it comes to surgical treatment for neck problems, two main options are available: Anterior Cervical Discectomy and Fusion (ACDF) and Cervical Artificial Disc Replacement (ADR). Both procedures aim to:
- Relieve nerve root or spinal cord compression
- Alleviate neck and/or arm pain
- Improve neck and/or arm function
However, there are key differences between the two, each with its own benefits and considerations.
In This Article:
- Artificial Disc Vs. Anterior Cervical Discectomy and Fusion
- Cervical Disc Replacement Surgery Video
- Anterior Cervical Discectomy and Fusion (ACDF) Video
What Are ACDF and Cervical ADR?
ACDF (Anterior Cervical Discectomy and Fusion) involves the complete removal of the problematic disc, which is then replaced with a bone graft (or bone graft substitute). Over time, the adjacent vertebrae fuse together, eliminating motion at the treated segment.
- Gold standard: ACDF is widely regarded as the gold standard for treating cervical degenerative disc disease and cervical disc herniation.
- No movement post-surgery: The fused segment becomes immobile, which may prevent future disc-related issues in that specific segment.
- Widely performed: ACDF has a long history, and most surgeons are highly experienced with this procedure.
Watch Anterior Cervical Discectomy and Fusion (ACDF) Video
Cervical ADR (Artificial Disc Replacement) involves removing the damaged disc and replacing it with an artificial disc implant designed to mimic the natural disc's function.
- Motion preservation: Unlike ACDF, ADR aims to maintain motion in the treated segment, which can help preserve the natural biomechanics of the cervical spine.
- Newer technique: Gaining popularity in the early 2000s, 1 Nunley PD, Coric D, Frank KA, Stone MB. Cervical Disc Arthroplasty: Current Evidence and Real-World Application. Neurosurgery. 2018;83(6):1087-1106. doi:10.1093/neuros/nyx579 ADR is considered a newer alternative to ACDF, though it has shown promising results.
Watch Cervical Disc Replacement Surgery Video
Both procedures are elective, meaning the patient has the option to choose whether or not to undergo surgery based on their specific condition and preferences.
advertisement
Spinal Levels Treated
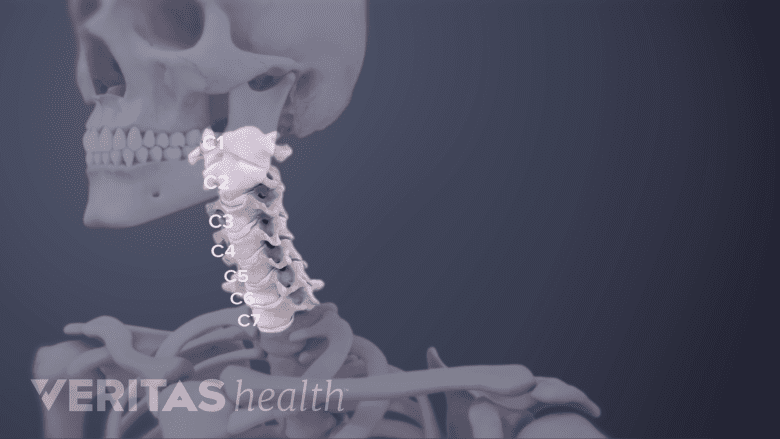
ACDF can be performed between C2 to C7, and ADR can be performed between C3 to C7.
ACDF can address nearly the entire cervical spine, from C2 to the C7-T1 level (where the neck meets the upper back). Up to four spinal levels can be treated with spinal fusion.
Cervical ADR is typically limited to treating damaged spinal discs between C3 and C7. Currently, ADR is generally approved for treating one or two levels, depending on the device and the patient's condition.
Surgical Techniques and Length of Hospital Stay
Both procedures are usually performed through an anterior (front) approach to the neck.
- Outpatient procedures: Single-level surgeries for both ACDF and ADR may be done on an outpatient basis, allowing the patient to return home the same or next day.
- Hospital stay: Multilevel surgeries may require an open surgical approach, often necessitating a hospital stay of 2-4 days.
Generally, ADR is associated with a shorter hospital stay compared to ACDF. 2 Paek S, Zelenty WD, Dodo Y, et al. Up to 10-year surveillance comparison of survivability in single-level cervical disc replacement versus anterior cervical discectomy and fusion in New York. Journal of Neurosurgery: Spine. Published online April 1, 2023:1-10. doi:https://doi.org/10.3171/2023.3.SPINE221377
advertisement
Surgical Success
Studies with long-term follow-up data show 3 Lavelle WF, Riew KD, Levi A, Florman JE. 10-year Outcomes of Cervical Disc Replacement with the BRYAN® Cervical Disc: Results from a Prospective, Randomized, Controlled Clinical Trial. Spine. 2018. DOI: 10.1097/BRS.0000000000002907 , 4 Burkus JK, Traynelis VC, Haid RW, Mummaneni PV. Clinical and radiographic analysis of an artificial cervical disc: 7-year follow-up from the Prestige prospective randomized controlled clinical trial: Clinical article. J Neurosurg Spine. 2014;21(4):516-28. DOI: 10.3171/2014.6.SPINE13996 , 5 Hisey MS, Zigler JE, Jackson R, et al. Prospective, Randomized Comparison of One-level Mobi-C Cervical Total Disc Replacement vs. Anterior Cervical Discectomy and Fusion: Results at 5-year Follow-up. Int J Spine Surg. 2016;10:10. DOI: 10.14444/3010 :
- Comparable outcomes: Both ACDF and cervical ADR demonstrate similar success rates in relieving neck and arm pain, improving arm function, and achieving patient satisfaction.
- High success rates: Over 70% of patients with degenerative disc disease at a single spinal level experience surgical success with either procedure.
- Biomechanics: Cervical ADR maintains more natural cervical spine biomechanics, potentially reducing stress on adjacent discs and lowering the risk of adjacent segment disease.
Possible Benefits of Cervical Artificial Disc Replacement
Some potential benefits of cervical ADR include:
- No bone graft risks: Unlike ACDF, ADR does not require a bone graft, eliminating risks like non-union or pain at the donor site.
- Quicker recovery: Patients often return to light work and daily activities within a week. Strenuous activities are typically resumed after about six weeks, compared to three months or longer for ACDF patients.
- Reduced risk of adjacent segment disease: By preserving motion, ADR reduces the risk of degeneration in adjacent spinal segments. 6 Spivak JM, Zigler JE, Philipp T, Janssen M, Darden B, Radcliff K. Segmental Motion of Cervical Arthroplasty Leads to Decreased Adjacent-Level Degeneration: Analysis of the 7-Year Postoperative Results of a Multicenter Randomized Controlled Trial. Int J Spine Surg. 2022;16(1):186-193. doi:10.14444/8187
See Recovery from Cervical Artificial Disc Replacement Surgery
Possible Benefits of ACDF
ACDF is a more widely used, simple procedure, with a larger pool of trained surgeons.
Some potential benefits of ACDF include:
- Wider range of patient eligibility: ACDF is suitable for a broader range of patients, including those with more complex spinal conditions, poor bone quality, or previous neck surgeries.
- Fewer unknown risks: ACDF has decades of data supporting its long-term safety and effectiveness. In contrast, the long-term durability of artificial discs is still being studied.
- Simpler procedure: ACDF is less complex, with more surgeons trained in this technique.
- Insurance coverage: ACDF is more commonly covered by insurance compared to ADR, although coverage for ADR is increasing.
See Anterior Cervical Discectomy and Fusion Complications
Choosing Between ACDF and Cervical ADR
Both procedures are safe and effective, but the choice between them depends on several factors, including:
- Patient’s age and overall health
- Condition of surrounding spinal structures
- Cause and severity of neck pain
- Number of spinal levels involved
- Patient’s lifestyle and preferences
- Surgeon’s experience and recommendation
advertisement
Emerging Research and Technologies
Newer advancements in spine surgery related to ADR and ACDF include:
- Hybrid procedures: Some patients may benefit from hybrid surgeries, combining ACDF and ADR, particularly when multiple levels are affected.
- Patient-specific implants: Advances in 3D printing and imaging are leading to patient-specific implants, potentially improving outcomes for both procedures.
Patient Involvement
It's crucial for patients to engage in detailed discussions with their surgeon, considering both the risks and benefits of each option, to make an informed decision that aligns with their long-term health goals.
- 1 Nunley PD, Coric D, Frank KA, Stone MB. Cervical Disc Arthroplasty: Current Evidence and Real-World Application. Neurosurgery. 2018;83(6):1087-1106. doi:10.1093/neuros/nyx579
- 2 Paek S, Zelenty WD, Dodo Y, et al. Up to 10-year surveillance comparison of survivability in single-level cervical disc replacement versus anterior cervical discectomy and fusion in New York. Journal of Neurosurgery: Spine. Published online April 1, 2023:1-10. doi:https://doi.org/10.3171/2023.3.SPINE221377
- 3 Lavelle WF, Riew KD, Levi A, Florman JE. 10-year Outcomes of Cervical Disc Replacement with the BRYAN® Cervical Disc: Results from a Prospective, Randomized, Controlled Clinical Trial. Spine. 2018. DOI: 10.1097/BRS.0000000000002907
- 4 Burkus JK, Traynelis VC, Haid RW, Mummaneni PV. Clinical and radiographic analysis of an artificial cervical disc: 7-year follow-up from the Prestige prospective randomized controlled clinical trial: Clinical article. J Neurosurg Spine. 2014;21(4):516-28. DOI: 10.3171/2014.6.SPINE13996
- 5 Hisey MS, Zigler JE, Jackson R, et al. Prospective, Randomized Comparison of One-level Mobi-C Cervical Total Disc Replacement vs. Anterior Cervical Discectomy and Fusion: Results at 5-year Follow-up. Int J Spine Surg. 2016;10:10. DOI: 10.14444/3010
- 6 Spivak JM, Zigler JE, Philipp T, Janssen M, Darden B, Radcliff K. Segmental Motion of Cervical Arthroplasty Leads to Decreased Adjacent-Level Degeneration: Analysis of the 7-Year Postoperative Results of a Multicenter Randomized Controlled Trial. Int J Spine Surg. 2022;16(1):186-193. doi:10.14444/8187

advertisement
Editor’s Top Picks
- Cervical Disc Replacement Surgery Video
- Potential Complications and Risks of Cervical Disc Replacement Surgery
- Anterior Cervical Discectomy and Fusion (ACDF) Video
- Anterior Cervical Discectomy and Fusion Complications
- What to Expect After ACDF Surgery
- Comparison of 2-Level Cervical Artificial Disc vs. 2 Level ACDF