
The natural cervical intervertebral disc is a remarkable mechanical structure from an engineering perspective. It has the ability to absorb a large compressive load while still providing an impressive range of motion between the bones in the neck.
Duplicating the natural disc's form and function with an artificial disc is challenging. However, several artificial cervical discs have been developed and are available as a surgical option to treat cervical disc problems that cause chronic neck pain and other symptoms, such as arm pain or weakness.
In This Article:
- Cervical Artificial Disc Replacement Surgery
- Considerations for Cervical Disc Replacement Surgery
- Surgical Procedure for Cervical Disc Replacement
- Recovery from Cervical Artificial Disc Replacement Surgery
- Potential Complications and Risks of Cervical Disc Replacement Surgery
- Cervical Disc Replacement Surgery Video
Goals for Cervical Artificial Disc Replacement
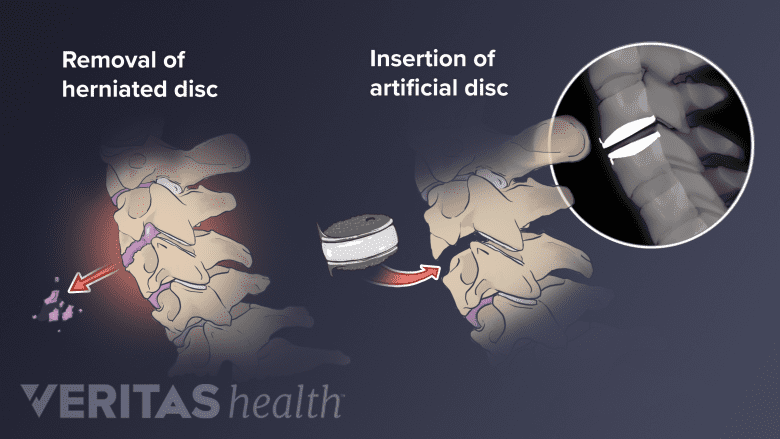
Artificial cervical disc replacement surgery replaces a damaged disc with an artificial one.
Before choosing to have cervical artificial disc replacement (ADR) surgery, also called cervical disc arthroplasty, it is important to understand what the surgery aims to accomplish. Key goals of cervical ADR include:
- Relieve nerve compression. When a disc herniates or begins to degenerate and collapse, there is less room for the nerve roots (and sometimes the spinal cord) to function, which can be a source of chronic pain, tingling, numbness, and/or weakness radiating from the neck into the arm. Clearing away the damaged disc and inserting an artificial disc aims to relieve pressure on any compressed nerves to give them space to heal and function normally. If the spinal cord was previously compressed, relieving pressure on it may help resolve or prevent progression of other symptoms, such as trouble with coordination, walking, and/or bladder or bowel control.
- Maintain motion at the repaired spinal level. By replacing the damaged disc with an artificial disc, natural biomechanics can be more closely retained throughout the cervical spine when the neck moves. While an artificial disc can help maintain motion, it does not create or improve motion. The cervical spine’s range of motion is unlikely to increase after disc replacement surgery.
It should be noted that any symptom relief achieved by cervical disc replacement surgery is primarily due to relieving nerve root inflammation and/or spinal cord compression. For this reason, cervical disc replacement surgery is not usually recommended for patients whose symptoms are limited to the neck.
Choosing Between an Artificial Disc and Fusion
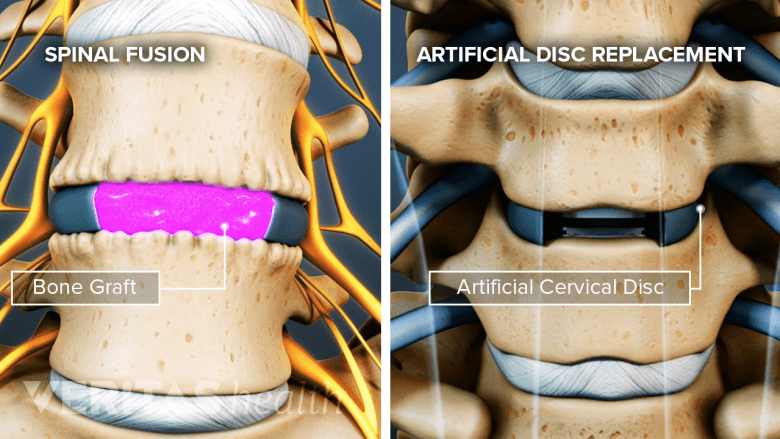
An artificial disc restores motion, and a spinal fusion eliminates motion in the spinal segment.
Anterior cervical discectomy and fusion (ACDF) surgery has long been considered the gold standard for treating pain and/or neurologic deficits stemming from nerve root inflammation and/or spinal cord compression in the cervical spine. While both ACDF and cervical ADR aim to remove a problematic disc and restore normal disc height, they differ in that ACDF fuses the adjacent vertebrae so motion is lost at that spinal level.
Watch Anterior Cervical Discectomy and Fusion (ACDF) Video
In cases when both ACDF and cervical ADR are viable options, some potential benefits of choosing an artificial disc may include:
- Maintaining more natural neck motion
- Reducing the risk for adjacent segments of the cervical spine to develop degenerative disc disease
- Eliminating potential complications and issues associated with the need for a bone graft and spinal instrumentation for spinal fusion
- Allowing quicker return to neck movement after surgery
There are also some considerations that could make ACDF a better option for some people. For example, there is more data available to back up the long-term safety and effectiveness of ACDF because it has been around for decades longer. Also, there are many cases where ACDF is an option but an artificial disc is not, such as when advanced spinal degeneration, bone weakness, or other serious underlying medical conditions are present.
See Artificial Disc Vs. Anterior Cervical Discectomy and Fusion
Efficacy of Cervical Artificial Disc Replacement Surgery
While cervical artificial disc replacement surgery is still considered a newer procedure, the data collected thus far have shown it to be relatively safe and effective for reducing neck and arm pain resulting from a compressed nerve root or spinal cord. Several randomized controlled trial studies, ranging from 2 to 10 years, have shown clinical success rates for cervical ADR to be similar or even better than ACDF clinical success rates. However, there is currently a lack of data on the success or failure of cervical ADR in the long run, such as over 15 or 20 years, which presents its own unknown risk and must be taken into consideration when deciding on the surgery. Current studies do demonstrate that the symptom relief achieved within the first few months after cervical ADR can last for many years.,,




