
Subscribe to our newsletter and get your FREE guide,
Natural Back Pain Relief: 16 Choices for Lasting Comfort.
Before making a decision about having surgery for adolescent idiopathic scoliosis, it is common for patients (and their parents) to have concerns and questions about what a spinal fusion might entail. In addition to questions about the surgery’s potential benefits, risks, and recovery period, it is normal to wonder what life will be like in the years afterward.
Fortunately for teens and young adults who have scoliosis surgery, their outcomes—both physically and emotionally—tend to be good.1Parsch D, Gaertner V, Brocai DRC, Carstens C. The effect of spinal fusion on the long-term outcome of idiopathic scoliosis. J Bone Joint Surg Br. 2001. 83(8): 1133-6.,2Zhang J, He D, Gao J, Yu X, Sun H, Chen Z, Li M. Spine (Phila Pa 1976). Changes in life satisfaction and self-esteem in patients with adolescent idiopathic scoliosis with and without surgical intervention. Spine (Phila Pa 1976). 2011; 36(9): 741-5.,3Benli IT, Ates B, Akalin S, Citak M, Kaya A, Alanay A. Minimum 10 years follow-up surgical results of adolescent idiopathic scoliosis patients treated with TSRH instrumentation. Eur Spine J. 2007; 16(3): 381-91. However, it is a major surgery and a big decision that should not be made without first considering all options. Scoliosis surgery is typically not considered unless bracing has been tried and failed to prevent the curve from reaching 45 or 50 degrees.
In This Article:
- Adolescent Idiopathic Scoliosis and Emotional Health
- How to Spot Depression in an Adolescent with Scoliosis
- When a Teen with Scoliosis Won’t Wear a Back Brace
- Long-Term Outlook for Adolescents Who Have Scoliosis Surgery
- Idiopathic Scoliosis Video
Patients Tend to Do Well in the Years After Scoliosis Surgery
The medical literature has closely followed short-term and long-term results of scoliosis surgery patients for many decades. As advances in technology have been made in surgical methods in recent decades, the outcomes have also been improving.
See Scoliosis Surgery Recovery: 3 Months Post-Operation and Beyond
For example, one small study in 2004 of young adults found that while scoliosis surgery patients had slightly lower physical health scores compared with peers who did not have scoliosis, their mental health scores were actually higher.4Kibsgård T, Brox JI, Reikerås O. Physical and mental health in young adults operated on for idiopathic scoliosis. J Orthop Sci. 2004. 9(4):360-3. Other studies have suggested that most patients are satisfied with scoliosis surgery’s results and go on to have productive lives similar to the rest of the population.3Benli IT, Ates B, Akalin S, Citak M, Kaya A, Alanay A. Minimum 10 years follow-up surgical results of adolescent idiopathic scoliosis patients treated with TSRH instrumentation. Eur Spine J. 2007; 16(3): 381-91.,5Asher MA, Burton DC. Adolescent idiopathic scoliosis: natural history and long term treatment effects. Scoliosis. 2006. 1:2.
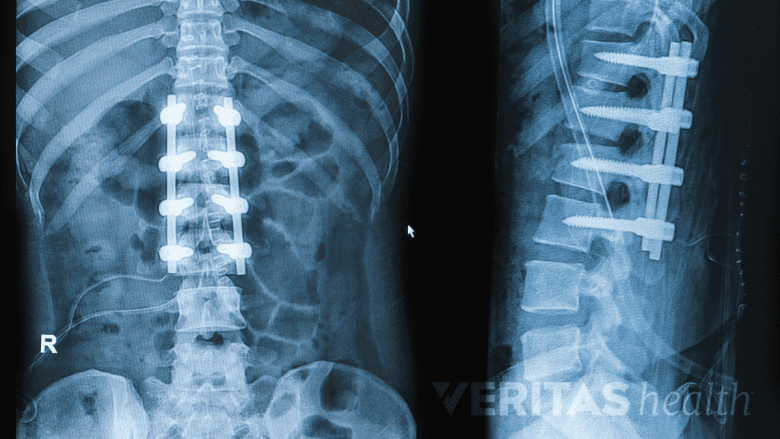
Older techniques for scoliosis surgery were associated with an elevated risk for back pain in the long run compared with people who did not have scoliosis surgery.5Asher MA, Burton DC. Adolescent idiopathic scoliosis: natural history and long term treatment effects. Scoliosis. 2006. 1:2. However, the newer techniques used today show promise for less long-term pain. A 2011 study performed the first 10-year follow-up on patients who had undergone a modern posterior fusion surgery for scoliosis and found that the healthy discs below the fusion level were holding up quite well—much better than some of the researchers had expected.6Green DW, Lawhorne TW, Widmann RF, et al. Long-term MRI follow-up demonstrates minimal transitional level lumbar disc degeneration after posterior spine fusion for adolescent idiopathic scoliosis. Spine (Phila Pa 1976). 2011. 36(23):1948-54.
Conversely, the medical literature clearly shows that if scoliosis goes untreated and worsens throughout adulthood into a severe deformity, it will lower quality of life compared with the general population. Some cases of untreated scoliosis are capable of progressing to the point of pushing against the heart and/or lungs, which could cause cardiopulmonary problems.5Asher MA, Burton DC. Adolescent idiopathic scoliosis: natural history and long term treatment effects. Scoliosis. 2006. 1:2.
advertisement
Why Surgery Should Not Be First Treatment Choice
Recovery from scoliosis surgery typically spans 6 to 12 months.
Some patients with idiopathic scoliosis are so frustrated with having any type of noticeable spinal deformity—even if it is small—that they want to go straight for surgery.
However, if the curve has not yet reached 45 degrees nor shown a likelihood of doing so, it will probably not progress into a severe deformity and surgery is usually not recommended. Some of the reasons include:
- Major surgery has risks. While scoliosis surgery is a relatively routine and safe procedure, it still involves the patient being sedated and the surgeon working in close proximity to the critically important and fragile spinal cord. Complications from scoliosis surgery are less likely today compared to a few decades ago, but risks still include infection, paralysis, the spine failing to fuse, more pain after the surgery than before, and others.
- Recovery from scoliosis surgery is challenging. In the first month or two following scoliosis surgery, the patient will be extremely limited in activities and required to manage the pain with medication. Full recovery takes 6 to 12 months, so it is not a process that should be taken lightly.
- Natural mobility of the spine is altered. Today’s scoliosis surgeries can usually be done without fusing as much of the back as in the past. However, a minor amount of spinal mobility is still likely to be lost.
advertisement
While it is not typically advised for patients with scoliosis curves at little to no risk of progressing past 45 degrees to have a spinal fusion, the surgery is still performed. If a patient is sufficiently bothered by the thought of his or her relatively small scoliosis curve, some surgeons might consider fusion surgery for cosmetic reasons.
- 1 Parsch D, Gaertner V, Brocai DRC, Carstens C. The effect of spinal fusion on the long-term outcome of idiopathic scoliosis. J Bone Joint Surg Br. 2001. 83(8): 1133-6.
- 2 Zhang J, He D, Gao J, Yu X, Sun H, Chen Z, Li M. Spine (Phila Pa 1976). Changes in life satisfaction and self-esteem in patients with adolescent idiopathic scoliosis with and without surgical intervention. Spine (Phila Pa 1976). 2011; 36(9): 741-5.
- 3 Benli IT, Ates B, Akalin S, Citak M, Kaya A, Alanay A. Minimum 10 years follow-up surgical results of adolescent idiopathic scoliosis patients treated with TSRH instrumentation. Eur Spine J. 2007; 16(3): 381-91.
- 4 Kibsgård T, Brox JI, Reikerås O. Physical and mental health in young adults operated on for idiopathic scoliosis. J Orthop Sci. 2004. 9(4):360-3.
- 5 Asher MA, Burton DC. Adolescent idiopathic scoliosis: natural history and long term treatment effects. Scoliosis. 2006. 1:2.
- 6 Green DW, Lawhorne TW, Widmann RF, et al. Long-term MRI follow-up demonstrates minimal transitional level lumbar disc degeneration after posterior spine fusion for adolescent idiopathic scoliosis. Spine (Phila Pa 1976). 2011. 36(23):1948-54.

advertisement