
Subscribe to our newsletter and get your FREE guide,
Natural Back Pain Relief: 16 Choices for Lasting Comfort.
Nonsurgical treatments may be helpful in relieving the symptoms of central canal stenosis. In general, nonsurgical treatments are considered when:
- Symptoms and signs of the central canal stenosis are mild (less severe)
- Stenosis of the central canal is mild
- The patient is older, and the surgical risks may outweigh the benefits
In such cases, nonsurgical treatments may be tried with close monitoring of the patient. In severe stenosis, when neurological symptoms interfere with daily living, surgery may be considered.
In This Article:
- Central Canal Stenosis
- Symptoms of Central Canal Stenosis
- Central Canal Stenosis Causes and Risk Factors
- Diagnosis of Central Canal Stenosis
- Nonsurgical Treatment of Central Canal Stenosis
- Surgery for Central Canal Stenosis
Common nonsurgical treatments for central canal stenosis include:
Physical Therapy
Neck extension exercises alleviate neck pain and enhance flexibility and strength.
Physical therapy under the guidance of a trained therapist is usually a part of the nonsurgical treatment regimen for stenosis of the central canal. Physical therapy typically involves an exercise program specifically formulated for the level of the spine that may be affected. In general, flexion-based exercises such as cycling or inclined walking may help open the central canal’s constrictors and improve blood flow to the spine.1Patel J, Osburn I, Wanaselja A, Nobles R. Optimal treatment for lumbar spinal stenosis: an update. Curr Opin Anaesthesiol. 2017;30(5):598-60
The goals for physical therapy may differ based on the spinal segment being treated.
- Physical therapy for cervical central canal stenosis mainly includes exercises to stabilize the cervical spine.1Patel J, Osburn I, Wanaselja A, Nobles R. Optimal treatment for lumbar spinal stenosis: an update. Curr Opin Anaesthesiol. 2017;30(5):598-60 These exercises include those involved in strengthening the muscles located at the:
- Back of the neck
- Upper back
- Back of the shoulder
- Physical therapy for thoracic and/or lumbar central canal stenosis includes exercises to improve the thoracic/lumbar spinal alignment.2Mo Z, Zhang R, Chang M, Tang S. Exercise therapy versus surgery for lumbar spinal stenosis: A systematic review and meta-analysis. Pak J Med Sci. 2018;34(4):879–885. doi:10.12669/pjms.344.14349 These exercises typically:
- Increase muscle tones around the thoracic and/or lumbar vertebrae
- Improve spinal stability
- Improve the posture of the lumbar spine in forward stooping
See Exercises for Lumbar Spinal Stenosis
While physical therapy for central canal stenosis exercises is not a cure, it may delay or reduce the risk for further debilitation. Also, the pain-relieving effects of physical therapy may not be immediate and may take a few days to weeks to start appearing.2Mo Z, Zhang R, Chang M, Tang S. Exercise therapy versus surgery for lumbar spinal stenosis: A systematic review and meta-analysis. Pak J Med Sci. 2018;34(4):879–885. doi:10.12669/pjms.344.14349 Studies show that the effects of physical therapy may improve the physical functioning of the spine, postponing surgery up to 1 year in some cases.1Patel J, Osburn I, Wanaselja A, Nobles R. Optimal treatment for lumbar spinal stenosis: an update. Curr Opin Anaesthesiol. 2017;30(5):598-60
advertisement
Medication
NSAIDs provide anti-inflammatory effects and help calm inflammation and pain in the neck.
Both prescription and over the counter (OTC) medications are used in treating stenosis pain. A few medications include1Patel J, Osburn I, Wanaselja A, Nobles R. Optimal treatment for lumbar spinal stenosis: an update. Curr Opin Anaesthesiol. 2017;30(5):598-60:
- Nonsteroidal anti-inflammatory drugs (NSAIDs) such as ibuprofen and aspirin
- Antiepileptic drugs such as gabapentin and pregabalin
- Prostaglandin analogues (to improve circulation) such as limaprost
With careful use, a short-term course of opioid medication may be helpful for severe episodes of nerve-related pain. It is essential that patients make sure their physician and pharmacist are aware of all their medications, supplements, and allergies in order to prevent side effects and drug interactions.
See Medications for Back Pain and Neck Pain
Injections
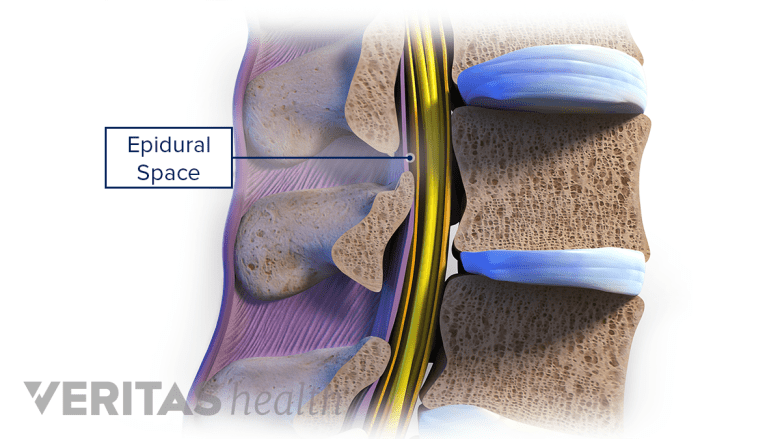
Epidural injections reduce inflammation and alleviate painful symptoms in central canal stenosis.
Injections to relieve stenosis pain are usually given in the epidural space (space outside the dura or outer lining of the spinal cord) or in the facet joints.
- Epidural injections. These injections mainly contain corticosteroids and may be given with or without a local anesthetic. Clinical trials show the pain-relieving effects of these injections may last from 3 to 12 months in stenosis.1Patel J, Osburn I, Wanaselja A, Nobles R. Optimal treatment for lumbar spinal stenosis: an update. Curr Opin Anaesthesiol. 2017;30(5):598-60
- Facet joint injections. Facet joint injections may contain steroids or anesthetic medications and are delivered in the facet joints of the vertebrae. Studies have shown the effects of facet joint injections to last up to 6 months in relieving facet pain in people with stenosis.3Zomalheto Z, Gounongbé M, Avimadjé M. Effect of facet joint injection in lumbar spinal stenosis: Experience of Rheumatology Hospital Unit of Cotonou (Benin). The Egyptian Rheumatologist. 2014;36(2):101-104. doi:10.1016/j.ejr.2013.10.001
Epidural and facet joint injections are usually given under x-ray guidance or fluoroscopy to direct the needle to the area of stenosis. A small amount of contrast dye is injected to confirm that the needle is in the desired spot before the medication is delivered.
Injecting steroids and other medications in the spine may have risks and complications such as bleeding, infection, nerve and/or spinal cord damage, and allergic reactions. It is important to discuss the benefits and potential risks of this treatment with a doctor before deciding to choose injections for central canal stenosis.
Read more about Injections for Neck and Back Pain Relief
Activity Modification
Patients are usually counseled to avoid activities that worsen their spinal stenosis symptoms. For lumbar stenosis, patients are typically more comfortable while bent (flexed) forward. Recommended activity modifications might include:
- Walking while bent over and leaning on a walker or shopping cart instead of walking upright
- Stationary biking while leaning forward on the handlebars instead of walking for exercise
- Sitting in a recliner instead of on a straight-back chair
Additionally, it is advised to avoid postural triggers for cervical stenosis pain. Wearing a neck brace intermittently during high activity periods may avoid unnecessary neck movements that cause pain.4Meyer F, Börm W, Thomé C. Degenerative cervical spinal stenosis: current strategies in diagnosis and treatment. Dtsch Arztebl Int. 2008;105(20):366–372. doi:10.3238/arztebl.2008.0366
advertisement
A less-studied treatment includes injecting stem cells or platelet-rich plasma to treat stenosis caused by degenerative disc disease.5Mohammed S, Yu J. Platelet-rich plasma injections: an emerging therapy for chronic discogenic low back pain. J Spine Surg. 2018;4(1):115–122. doi:10.21037/jss.2018.03.04,6Sivakamasundari V, Lufkin T. Stemming the Degeneration: IVD Stem Cells and Stem Cell Regenerative Therapy for Degenerative Disc Disease. Adv Stem Cells. 2013;2013:724547. doi:10.5171/2013.724547These regenerative therapies, however, are still in research phases, and more time is needed until their efficacy in treating spinal stenosis can be established.
In cases where neurological deficits are present, such as weakness or numbness, spinal stenosis surgery may be considered. Surgical techniques may vary based on the level of the spine being treated.
- 1 Patel J, Osburn I, Wanaselja A, Nobles R. Optimal treatment for lumbar spinal stenosis: an update. Curr Opin Anaesthesiol. 2017;30(5):598-60
- 2 Mo Z, Zhang R, Chang M, Tang S. Exercise therapy versus surgery for lumbar spinal stenosis: A systematic review and meta-analysis. Pak J Med Sci. 2018;34(4):879–885. doi:10.12669/pjms.344.14349
- 3 Zomalheto Z, Gounongbé M, Avimadjé M. Effect of facet joint injection in lumbar spinal stenosis: Experience of Rheumatology Hospital Unit of Cotonou (Benin). The Egyptian Rheumatologist. 2014;36(2):101-104. doi:10.1016/j.ejr.2013.10.001
- 4 Meyer F, Börm W, Thomé C. Degenerative cervical spinal stenosis: current strategies in diagnosis and treatment. Dtsch Arztebl Int. 2008;105(20):366–372. doi:10.3238/arztebl.2008.0366
- 5 Mohammed S, Yu J. Platelet-rich plasma injections: an emerging therapy for chronic discogenic low back pain. J Spine Surg. 2018;4(1):115–122. doi:10.21037/jss.2018.03.04
- 6 Sivakamasundari V, Lufkin T. Stemming the Degeneration: IVD Stem Cells and Stem Cell Regenerative Therapy for Degenerative Disc Disease. Adv Stem Cells. 2013;2013:724547. doi:10.5171/2013.724547

advertisement