
Subscribe to our newsletter and get your FREE guide,
Natural Back Pain Relief: 16 Choices for Lasting Comfort.
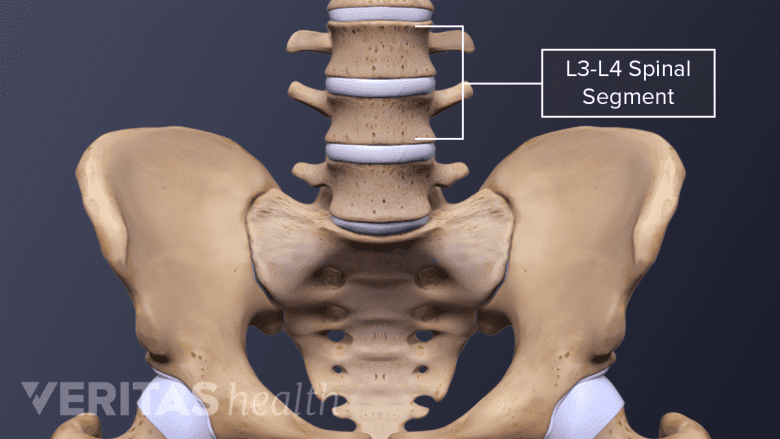
The L3-L4 spinal motion segment, positioned in the middle of the lumbar spine, plays an important role in supporting the weight of the torso and protecting the cauda equina (nerves that descend from the spinal cord). While the L3-L4 motion segment is less likely to be injured compared to its lower counterparts, it may be subject to degeneration, trauma, and disc-related problems.
In This Article:
- All About the L3-L4 Spinal Segment
- L3-L4 Treatment
- Spinal Motion Segment: L3-L4 Animation
Anatomy of the L3-L4 Spinal Motion Segment
The L3-L4 motion segment includes the following structures:
L3 and L4 vertebrae
An injured L3-L4 motion segment may cause pain, numbness, or weakness in the lower back or legs.
Each vertebra consists of a vertebral body in front and a vertebral arch at the back with the following characteristics:
- The height of the vertebral body of L3 is equal in the front and back; L4 is taller in front compared to the back.1Cramer GD. The Lumbar Region. In: Clinical Anatomy of the Spine, Spinal Cord, and Ans. Elsevier; 2014:246-311. doi:10.1016/b978-0-323-07954-9.00007-4,2Wilke H-J, Volkheimer D. Basic Biomechanics of the Lumbar Spine. In: Biomechanics of the Spine. Elsevier; 2018:51-67. doi:10.1016/b978-0-12-812851-0.00004-5
- The vertebral arch has 3 bony protrusions: a prominent spinous process in the middle and two transverse processes on either side. L3 has the longest spinous process in the lumbar region.1Cramer GD. The Lumbar Region. In: Clinical Anatomy of the Spine, Spinal Cord, and Ans. Elsevier; 2014:246-311. doi:10.1016/b978-0-323-07954-9.00007-4
- The region between the spinous process and the transverse process is called the lamina. The region between the transverse process and the vertebral body is called the pedicle.
- The L3 and L4 vertebrae are connected at the back by a pair of facet joints (zygapophyseal joints), which are covered by articulating cartilage to provide smooth movements between the joint surfaces.
L3-L4 intervertebral disc
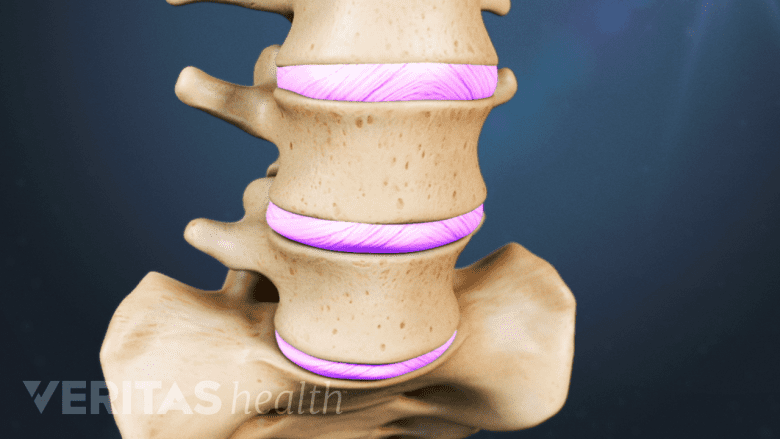
The spinal discs provide flexibility and support for the spine.
A disc made of a soft, gelatinous core (nucleus pulposus) surrounded by tough layers of fibrous tissue (annulus fibrosus) is situated between the vertebral bodies of L3 and L4. This disc provides cushioning and shock-absorbing functions to protect the vertebrae from grinding against each other during spinal movements.
Watch Lumbar Disc Anatomy Animation
L3 spinal nerve
The L3 spinal nerve roots exit the cauda equina through small bony openings (intervertebral foramina) on the left and right sides of the spinal canal. The L3 nerve innervates specific areas of skin and muscles in the lower limbs.
- The L3 dermatome is an area of skin that receives sensations through the L3 spinal nerve and includes the front part of the thigh and inner part of the leg.
- The L3 myotome is a group of muscles controlled by the L3 spinal nerve and includes parts of specific muscles in the hip, thigh, and leg.
The L3-L4 motion segment provides a bony enclosure to protect the cauda equina and other delicate structures.
advertisement
Common Conditions Affecting the L3-L4 Spinal Segment

The L3-L4 disc may degenerate or herniate due to age-related changes or from trauma.
Potential problems that may occur at the L3-L4 motion segment are:
- Osteoarthritis. The L3-L4 facets are typically subject to recurrent rotational strain, which may cause osteoarthritis to develop in these joints, resulting in facet joint pain.1Cramer GD. The Lumbar Region. In: Clinical Anatomy of the Spine, Spinal Cord, and Ans. Elsevier; 2014:246-311. doi:10.1016/b978-0-323-07954-9.00007-4
- Degenerative spondylolisthesis. Age-related changes in the facet joints may result in the forward slippage of the L3 vertebra over L4.1Cramer GD. The Lumbar Region. In: Clinical Anatomy of the Spine, Spinal Cord, and Ans. Elsevier; 2014:246-311. doi:10.1016/b978-0-323-07954-9.00007-4
- Disc problems. The L3-L4 disc may degenerate or herniate due to age-related changes or from trauma.
When subject to acute trauma, the L3-L4 motion segment may rarely undergo facet joint dislocation, fracture, and/or damage to the cauda equina. Rarely, tumors and infections may affect the L3-L4 motion segment.
Symptoms and Signs Stemming from L3-L4

Injured L3-L4 motion segments may cause symptoms of pain, numbness or weakness in the lower back or legs.
The L3-L4 motion segment may cause muscle pain, discogenic pain, radicular (nerve root) pain, and/or radiculopathy (neurologic deficit) that typically affects the lower back and/or the legs.
When the L3 spinal nerve is involved, the following symptoms may occur:
- Sharp pain, typically felt as a shooting and/or burning feeling that may occur in the thigh and/or inner part of the leg. 3Dulebohn SC, Ngnitewe Massa R, Mesfin FB. Disc Herniation. [Updated 2019 Aug 1]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2019 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK441822/
- Numbness in the thigh and/or inner part of the leg.3Dulebohn SC, Ngnitewe Massa R, Mesfin FB. Disc Herniation. [Updated 2019 Aug 1]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2019 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK441822/
- Weakness while moving the thigh and/or knee in different directions.3Dulebohn SC, Ngnitewe Massa R, Mesfin FB. Disc Herniation. [Updated 2019 Aug 1]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2019 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK441822/
- Abnormal sensations, such as a feeling of pins-and-needles and/or tingling.
These symptoms are typically experienced in one leg. Rarely, both legs may be affected together.
Read more about Lumbar Radiculopathy
advertisement
An injury to the cauda equina is called cauda equina syndrome. This syndrome is characterized by weakness, numbness, tingling, and /or paralysis in both legs. There may also be a reduction or complete loss of bowel and/or bladder control. Immediate medical attention is crucial in this condition to preserve leg function.
Nonsurgical treatments are often tried first to treat the conditions originating from L3-L4, except for cauda equina syndrome, which must have urgent surgical consultation. In rare cases, surgery may be considered.
- 1 Cramer GD. The Lumbar Region. In: Clinical Anatomy of the Spine, Spinal Cord, and Ans. Elsevier; 2014:246-311. doi:10.1016/b978-0-323-07954-9.00007-4
- 2 Wilke H-J, Volkheimer D. Basic Biomechanics of the Lumbar Spine. In: Biomechanics of the Spine. Elsevier; 2018:51-67. doi:10.1016/b978-0-12-812851-0.00004-5
- 3 Dulebohn SC, Ngnitewe Massa R, Mesfin FB. Disc Herniation. [Updated 2019 Aug 1]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2019 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK441822/

advertisement