
Subscribe to our newsletter and get your FREE guide,
Natural Back Pain Relief: 16 Choices for Lasting Comfort.
Surgical treatment is indicated when lumbar spinal stenosis causes severe leg pain and constant or progressive neurologic signs, such as numbness and weakness. Several weeks or months of nonsurgical treatments are typically tried before considering surgery.
In This Article:
- Lumbar Spinal Stenosis
- Lumbar Spinal Stenosis Symptoms
- Lumbar Spinal Stenosis Causes and Diagnosis
- Lumbar Spinal Stenosis Treatment
- Lumbar Spinal Stenosis Surgery Options
- Lumbar Spinal Stenosis Video
Research indicates that up to 90% of patients may experience some relief from neurological symptoms after surgery. 1 Lee SY, Kim TH, Oh JK, Lee SJ, Park MS. Lumbar Stenosis: A Recent Update by Review of Literature. Asian Spine J. 2015;9(5):818–828. doi:10.4184/asj.2015.9.5.818 In medical emergencies, such as for certain tumors, infections, cauda equina syndrome, or conus medullaris syndrome, surgery may be important to prevent nerve damage and preserve leg function.
Types of Surgical Procedures for Lumbar Spinal Stenosis
Spinal surgery to treat lumbar stenosis may be done using minimally invasive techniques or by open surgical methods. The main goal of surgery is to decompress the neural structures and provide more room for the spinal cord, cauda equina, and/or nerve roots.
Decompression surgeries

The lamina, facet joint, and/or intervertebral foramen is surgically treated to provide more space for compressed spinal nerves.
Depending on the level and severity of the stenosis, the following decompression procedures may be performed:
- Laminectomy. One or both laminae (the posterior, or back, part of the vertebra) are removed to provide more space for the compressed spinal cord and/or nerve roots.
See Lumbar Laminectomy Surgery for Spinal Stenosis (Open Decompression)
- Laminotomy. A part of or the entire lamina on one side of the affected vertebra is removed with or without adjacent tissues.
- Foraminotomy. The opening for the spinal nerve (intervertebral foramen) is enlarged by removing bony overgrowth.
- Facetectomy. The facet joints are typically trimmed, undercut, or removed to relieve nerve root pressure.
advertisement
As appropriate, these procedures may be combined and performed at the same time. For example, a laminectomy procedure may be done along with a foraminotomy, and the surgery is called a laminoforaminotomy. Additional procedures may be done in combination with the above, such as hypertrophic (overgrown) ligament removal.
When more than one spinal level is treated and there is a possibility for decreased stability in the motion segment, a spinal fusion may be performed to fuse the adjacent vertebrae together.
Interspinous spacers
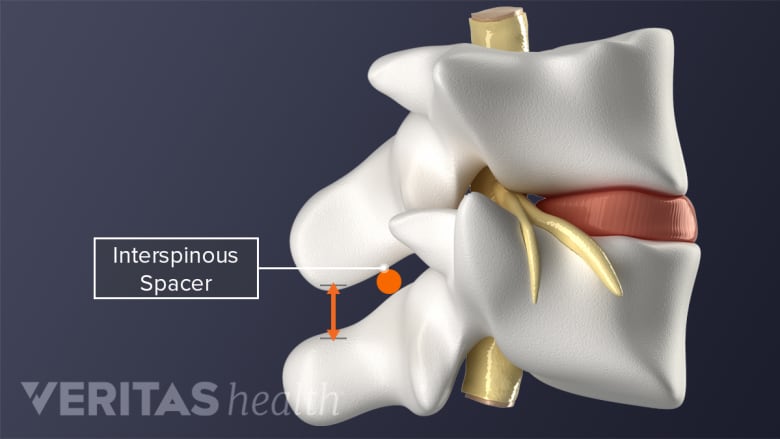
The interspinous spacers may prevent the narrowing of bony openings for nerves.
Specialized devices may be surgically inserted between the spinous processes (bony protrusion at the back of the vertebra) of adjacent vertebrae to provide more space between the vertebrae. These spacers typically prevent narrowing of the bony openings for nerves during spinal loading from regular movement. 2 Lurie J, Tomkins-Lane C. Management of lumbar spinal stenosis. BMJ. January 2016:h6234. doi:10.1136/bmj.h6234
Minimally invasive techniques may be used to perform this procedure.
Spinal cord stimulation
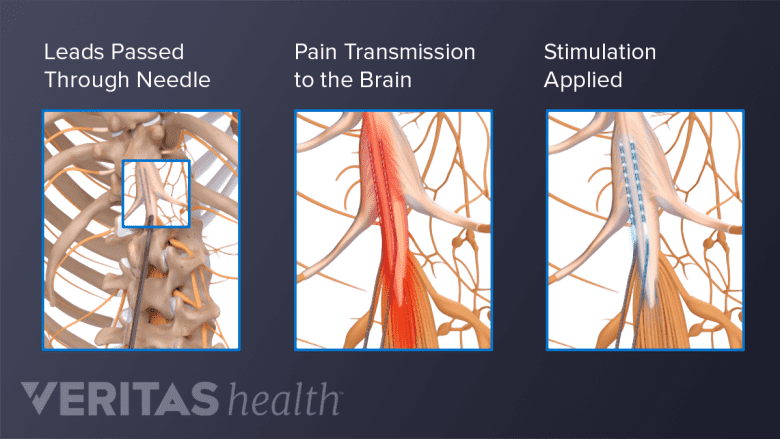
Spinal cord stimulation may alleviate lumbar spinal stenosis pain by interrupting the pain signals.
Limited data suggest that spinal cord stimulation therapy may help control lumbar spinal stenosis pain. 3 Patel J, Osburn I, Wanaselja A, Nobles R. Optimal treatment for lumbar spinal stenosis. Current Opinion in Anaesthesiology. 2017;30(5):598-603. doi:10.1097/aco.0000000000000495 Spinal cord stimulation directs mild electrical pulses through a small, implanted device in the lower back. These impulses interfere with pain messages, preventing them from reaching the brain.
Watch Spinal Cord Stimulation for Chronic Back Pain Video
Factors that May Contribute to a Successful Surgical Outcome

Symptoms limited to one leg may be easier to treat compared to both legs.
Presence of the following factors typically provide favorable outcomes after a lumbar spinal stenosis surgery 1 Lee SY, Kim TH, Oh JK, Lee SJ, Park MS. Lumbar Stenosis: A Recent Update by Review of Literature. Asian Spine J. 2015;9(5):818–828. doi:10.4184/asj.2015.9.5.818 :
- When the stenosis is present at a single spinal level
- Neurologic deficits, such as weakness, are of less than 6 weeks duration
- The symptoms are limited to one leg
- The symptoms are relieved by postural change, such as bending forward
For surgery to be successful, there must be a structural condition (such as a hypertrophied ligament or bone spur) that is known to respond to surgical treatment.
Factors that may adversely affect surgical outcomes include the use of tobacco products, excessive alcohol and/or drug intake, inability to tolerate or cope with the surgical procedure (due to age and/or general health), and the presence of other medical conditions.
advertisement
As with any surgery, there are potential risks, including but not limited to nerve or spinal cord damage, bleeding, infection, clot formation, and continued symptoms post-surgery.
See Laminectomy and Spinal Stenosis: Risks and Complications
Spinal surgery is elective, which means it is the patient’s choice to have surgery or not. A patient’s decision to consent for surgery is typically based on the amount of pain and dysfunction that they experience, symptoms’ effect on daily activities, and their ability to cope with the procedure. It is important that the patient understands the risks, benefits, and alternatives of the procedure and that any questions they have are answered to their satisfaction.
- 1 Lee SY, Kim TH, Oh JK, Lee SJ, Park MS. Lumbar Stenosis: A Recent Update by Review of Literature. Asian Spine J. 2015;9(5):818–828. doi:10.4184/asj.2015.9.5.818
- 2 Lurie J, Tomkins-Lane C. Management of lumbar spinal stenosis. BMJ. January 2016:h6234. doi:10.1136/bmj.h6234
- 3 Patel J, Osburn I, Wanaselja A, Nobles R. Optimal treatment for lumbar spinal stenosis. Current Opinion in Anaesthesiology. 2017;30(5):598-603. doi:10.1097/aco.0000000000000495

advertisement