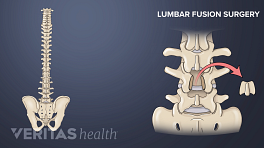
An Anterior Lumbar Interbody Fusion (ALIF) surgery is a type of spinal fusion performed to stabilize a painful motion segment in the lower back, commonly caused by lumbar degenerative disc disease and/or spondylolisthesis. The surgical approach is via the abdomen, to access the front–or the “anterior”–of the spine, where the disc is located.

Doctors Lane and Moore first performed an ALIF surgery in the 1940s for the treatment of lower back pain. 1 Lane JD Jr, Moore ES Jr. Transperitoneal approach to the intervertebral disc in the lumbar area. Ann Surg. 1948;127:537–551. The procedure did not gain immediate favor because of low success rates; about 36% to 52% of patients found significant pain relief and about 32% to 56% had a successful fusion of vertebral bones. 2 Kunc Z, Sourek K, Bret J. Transabdominal anterior interbody fusion of spondylolisthesis L5-S1. Acta Neurol Scand. 1970;46(3):354-368. doi:10.1111/j.1600-0404.1970.tb05800.x , 3 Stauffer RN, Coventry MB. Anterior interbody lumbar spine fusion. Analysis of Mayo Clinic series. J Bone Joint Surg Am. 1972;54(4):756-768.
Starting in the 1990s, however, there was a resurgence of popularity for anterior lumbar interbody fusion surgery because of the advent of new threaded titanium cages that held the disc space better and allowed for a higher fusion rate. Success rates of ALIF are now about 95%, 4 Jackson KL, Yeoman C, Chung WM, Chappuis JL, Freedman B. Anterior lumbar interbody fusion: two-year results with a modular interbody device. Asian Spine J. 2014;8(5):591-598. doi:10.4184/asj.2014.8.5.591 making ALIF a common approach for eligible cases of low back pain.
In This Article:
- Anterior Lumbar Interbody Fusion (ALIF) Surgery
- Potential Risks and Complications with ALIF Surgery
- ALIF (Anterior Lumbar Interbody Fusion) Video
Modern Applications of ALIF Surgery
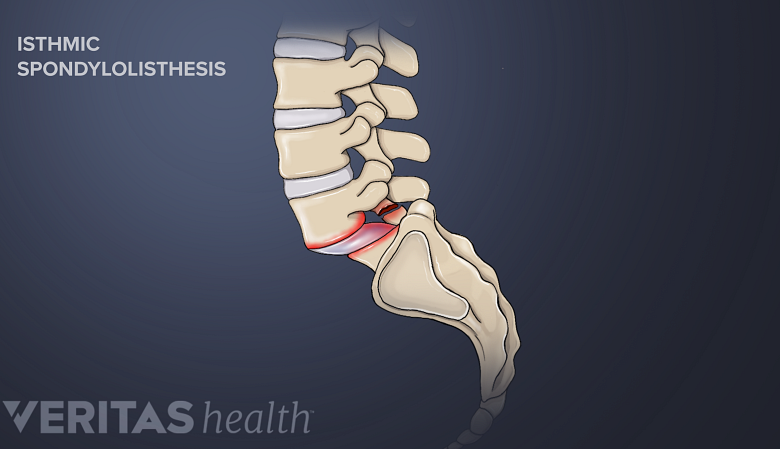
Isthmic spondylolisthesis may be indicated for an anterior-posterior fusion surgery.
An ALIF alone can be sufficient in cases where there is not a lot of instability. ALIF is preferred in cases of:
- Single-level degenerative disc disease with disc space collapse
- Multi-level fusion and disc removal
- Lumbosacral fusion
The anterior approach can also be useful in treating a failed posterior fusion–when the posterior approach (from the back) to spinal fusion surgery is unsuccessful and causes pain.
An anterior approach combined with a posterior approach (anterior/posterior fusions) provides a more rigid fixation of vertebrae than an anterior approach alone. Clinical examples that require a combined approach include:
- A “tall” disc
- Isthmic spondylolisthesis
ALIF with posterior instrumentation and fusion provides additional stability to the fused level of the spine.
Description of Anterior Lumbar Interbody Fusion (ALIF) Surgery
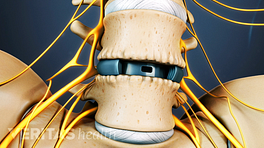
Bone graft aids in the growth of new bone and helps fuse the spinal motion segment.
The anterior lumbar interbody fusion is similar to the posterior lumbar interbody fusion (PLIF), except that in ALIF, the disc space is fused by approaching the spine through the abdomen instead of through the lower back. Over the course of about 2 hours, the surgeon will perform the following initial steps.
- Making the incision. A 3-inch to 5-inch vertical incision is made in the lower abdomen, just left of the line from the pubic area to the belly button.
- Accessing the peritoneum. Layers of fat and muscle must be crossed to reach the peritoneum, which is a large sack that holds the internal organs in place.
There are 2 ways to achieve access to the front of the spine.
- The transperitoneal is an approach that may be used when fusing the L4-L5 or L5-S1 segments. This approach may be preferred for surgical patients who are obese. In this procedure, the fat layer is dissected until the peritoneal membrane is accessed. The forceps lift the fat layer, taking the peritoneal membrane with it. This method is designed to gently separate the peritoneal membrane from the internal organs. 5 Laratta JL, Davis EG, Glassman SD, Dimar JR. The transperitoneal approach for anterior lumbar interbody fusion at L5-S1: a technical note. J Spine Surg. 2018;4(2):459-460. doi:10.21037/jss.2018.05.18
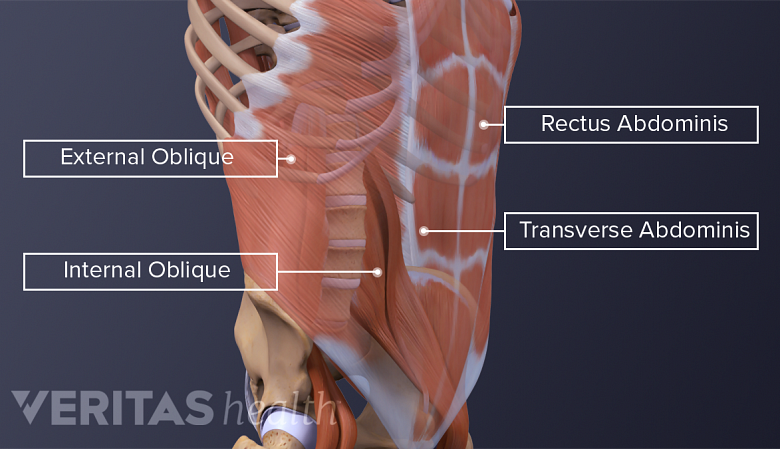
- The retroperitoneal approach tends to be the most common method because it may be used in the fusion of any of the lumbar spine segments. Conventionally, this method involves cutting the topmost muscular layer (the external oblique abdominal muscle) along the fibers and cauterizing the remaining layers.
Another emerging alternative involves splitting all 3 layers of abdominal muscle (the external oblique, internal oblique, and transverse muscles) along the fibers to reach the spine. 6 Saraph V, Lerch C, Walochnik N, Bach CM, Krismer M, Wimmer C. Comparison of conventional versus minimally invasive extraperitoneal approach for anterior lumbar interbody fusion. Eur Spine J. 2004;13(5):425-431. doi:10.1007/s00586-004-0722-4
The remaining steps include:
- Retracting the peritoneum. The peritoneum can be retracted to the side, allowing the spine surgeon access to the front of the spine without actually entering the abdomen.
- Retracting blood vessels. On top of the spine lay large blood vessels that continue to the legs. Many spine surgeons will perform this surgery together with a vascular surgeon, who mobilizes these large blood vessels.
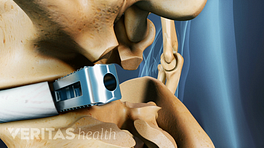
- Replacing the disc with the bone graft. After the blood vessels have been moved aside, the disc material is removed and bone grafts or anterior interbody cages with bone graft are inserted. Another incision may be needed from the back to help fixate the devices. Pedicle screws, which always accompany PLIF surgery, may be optional during ALIF surgery.
Patients typically stay in the hospital for 1 night, sometimes 2 nights, and then return home. A full recovery plan will be recommended and usually focuses on rehabilitation for the 6- to 12-week period following the surgery.
See Postoperative Care for Spinal Fusion Surgery
The fusion process for the bones does not occur during the surgery itself; instead, the surgery sets up the environment for the bones to fuse and over the following months (up to 12 months) the fusion gradually takes place. It is important to schedule follow-up appointments to evaluate the progress of the fusion.
Watch Video: Stages of Bone Healing in Lumbar Spine Fusion Surgery
Advantages of ALIF Surgery
The ALIF approach offers the benefit of minimal disruption to back muscles and nerves.
The ALIF approach is just one of several approaches to spinal fusion. The primary benefit of using the ALIF approach is the direct access to the front of the spinal column.
Relative to other fusion approaches, benefits of choosing the ALIF approach include:
- Back muscles and nerves remain undisturbed
- A large spacer (spinal implant) may be used for enhanced stability of the fusion construct
- The bone graft is placed in compression against a large surface area of the endplates
- The natural curvature of the spine can be restored more efficiently and effectively
There are certain disadvantages to the anterior approach as well. For example, there is a risk of hernia after ALIF surgery. Whether a spine surgeon approaches the disc space from an anterior approach or from one of the posterior approaches (PLIF or TLIF) is largely dependent on how comfortable the surgeon is with the anterior approach and operating around the aorta and vena cava, which are large blood vessels attached to the heart.
Most spine surgeons have not had a great deal of experience doing the procedure by themselves, and not all spine surgeons have access to a skilled vascular surgeon to help them with the approach. Therefore, a posterior approach for lumbar spine fusion surgery may be more practical for many surgeons.
- 1 Lane JD Jr, Moore ES Jr. Transperitoneal approach to the intervertebral disc in the lumbar area. Ann Surg. 1948;127:537–551.
- 2 Kunc Z, Sourek K, Bret J. Transabdominal anterior interbody fusion of spondylolisthesis L5-S1. Acta Neurol Scand. 1970;46(3):354-368. doi:10.1111/j.1600-0404.1970.tb05800.x
- 3 Stauffer RN, Coventry MB. Anterior interbody lumbar spine fusion. Analysis of Mayo Clinic series. J Bone Joint Surg Am. 1972;54(4):756-768.
- 4 Jackson KL, Yeoman C, Chung WM, Chappuis JL, Freedman B. Anterior lumbar interbody fusion: two-year results with a modular interbody device. Asian Spine J. 2014;8(5):591-598. doi:10.4184/asj.2014.8.5.591
- 5 Laratta JL, Davis EG, Glassman SD, Dimar JR. The transperitoneal approach for anterior lumbar interbody fusion at L5-S1: a technical note. J Spine Surg. 2018;4(2):459-460. doi:10.21037/jss.2018.05.18
- 6 Saraph V, Lerch C, Walochnik N, Bach CM, Krismer M, Wimmer C. Comparison of conventional versus minimally invasive extraperitoneal approach for anterior lumbar interbody fusion. Eur Spine J. 2004;13(5):425-431. doi:10.1007/s00586-004-0722-4