The vast majority of thoracic herniated disc symptoms can be treated without thoracic surgery. There are a variety of non-surgical treatment options that can be tried, and often patients will need to try several, or a combination of different treatments, to find what works best for them.
In This Article:
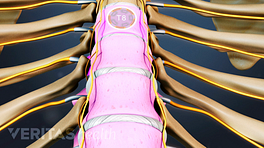
Non-Surgical Treatments for Thoracic Herniated Discs
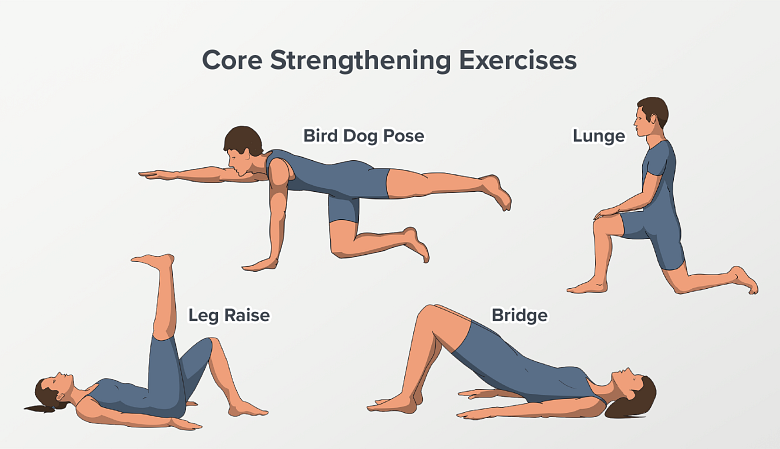
Core strengthening exercises aim to strengthen the spine and relieve back pain.
Non-surgical treatment options for symptoms of a thoracic herniated disc will typically include one or a combination of the following:
- A short period of rest (e.g. one or two days) and activity modification (eliminating the activities and positions that worsen or cause the thoracic back pain). After a short period or rest, the patient should return to activity as tolerated. Gentle exercise, such as walking, is a good way to return to activity. See 5 Exercises for Upper and Middle Back Pain
- Narcotic and non-narcotic analgesic medications to help reduce the thoracic back pain. Narcotic pain medication is usually only prescribed to treat severe upper back pain for a short period of time. For mild or moderate thoracic back pain, an over-the-counter pain reliever such as acetaminophen (e.g. Tylenol) is commonly recommended for thoracic herniated discs.
- Anti-inflammatory agents, to help reduce inflammation around the herniated disc in the upper back, including:
- Medications (NSAIDs - such as ibuprofen or a COX-2 inhibitor, or oral steroids)
- Anti-inflammatory injections (such as an epidural steroid injection)
- Ice packs (applied to the painful area for 15–20 minutes at a time, as often as necessary)
- Manual manipulation (usually performed by a chiropractor or an osteopathic doctor)
- Strengthening exercises (such as core stabilization exercises)
The patient’s activity levels should be progressed gradually over a 6 to 12 week period as symptoms improve. In the vast majority of cases, the natural history of thoracic disc herniation is one of improvement with one or a combination of the above conservative (non-operative) treatments.