A multilevel fusion surgery involves the removal of the disc and fusion of the spinal bones (vertebrae) with a bone graft to achieve stability of the spinal segment and eliminate motion. Additionally, the facet joints may be fused at the back of the motion segment to further restrict movement within the segment.
In This Article:
- Multilevel Spinal Fusion for Low Back Pain
- The Multilevel Spinal Fusion Surgery
- Multilevel Fusion Risks
- Recovery After Fusion at More Than One Level
- Multi-level Spinal Fusion Video
Interbody Fusion in Multilevel Spinal Surgery
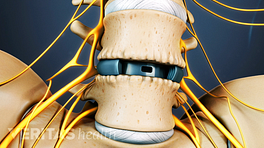
When fusion is achieved by removing the spinal disc and filling the space with a bone graft to facilitate bone growth and fusion, the procedure is called interbody fusion. A metal or plastic spacer (interbody cage) is commonly placed into the disc space in addition to the bone graft, in order to maintain the height of the disc during healing.
Lumbar interbody fusion can be accomplished through several approaches, including:
Anterior lumbar interbody fusion
An anterior lumbar interbody fusion (ALIF) stabilizes a painful lower back motion segment through spinal fusion.
An anterior lumbar interbody fusion (ALIF) surgery is a type of spinal fusion performed to stabilize a painful motion segment in the lower back, commonly caused by lumbar degenerative disc disease and/or spondylolisthesis. The surgical approach is via the front of the abdomen, working around and behind the abdominal contents to access the front of the spine, where the disc is located. ALIF is a common surgical technique used to treat lumbar degenerative disc disease with disc collapse, and spondylolisthesis.
Extreme lumbar interbody fusion
An extreme lumbar interbody fusion (XLIF) approach is used to place a large cage to fill the disc space directly from the side of the disc, through a split in the psoas muscle present alongside the lumbar spine. The incision is on the side of the body, and the approach stays behind all the abdominal organs. It can only be used at the L1-L2, L2-L3, L3-L4, and L4-L5 levels. It is not used at the L5-S1 level due to the position of the pelvis. A slightly anterior modification of this approach is called the oblique lumbar interbody fusion (OLIF).
XLIF surgery may also be referred to as lateral lumbar interbody fusion (LLIF) or direct lateral interbody fusion (DLIF).
See Description of XLIF Surgery
Posterior lumbar interbody fusion
Posterior lumbar interbody fusion (PLIF) aims to fuse two levels of the spine by taking a surgical approach from behind the lumbar spine. The nerve sac must be exposed and retracted to make room for smaller cages than can be placed through the anterior or lateral approaches. Conditions treated using this approach include degenerative disc disease with spinal instability, recurrent disc herniation, spondylolisthesis, and spinal stenosis. 1 Mobbs RJ, Phan K, Malham G, Seex K, Rao PJ. Lumbar interbody fusion: techniques, indications and comparison of interbody fusion options including PLIF, TLIF, MI-TLIF, OLIF/ATP, LLIF and ALIF. J Spine Surg. 2015;1(1):2-18. doi:10.3978/j.issn.2414-469X.2015.10.05
Transforaminal lumbar interbody fusion
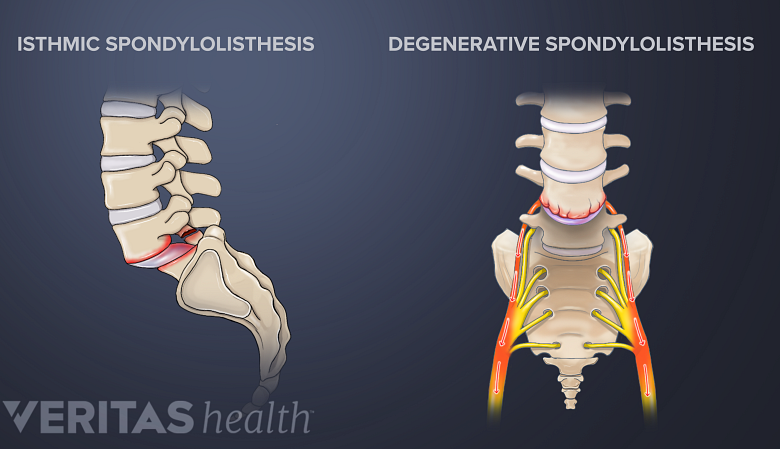
A TLIF surgery may be indicated when back and/or leg pain occurs due to spondylolisthesis.
The transforaminal lumbar interbody fusion (TLIF) technique is used to place an interbody cage via an oblique insertion approach, typically by removing one of the facet joints. A TLIF surgery may be indicated when back and/or leg pain occurs due to spondylolisthesis, degenerative disc disease, recurrent disc herniations, or pseudoarthrosis (the lack of a solid fusion) from prior fusion surgery. 1 Mobbs RJ, Phan K, Malham G, Seex K, Rao PJ. Lumbar interbody fusion: techniques, indications and comparison of interbody fusion options including PLIF, TLIF, MI-TLIF, OLIF/ATP, LLIF and ALIF. J Spine Surg. 2015;1(1):2-18. doi:10.3978/j.issn.2414-469X.2015.10.05
See TLIF Back Surgery Success Rates and Risks
Posterior or Posterolateral Fusion in Multilevel Spinal Surgery
This approach is done through the back and focuses on connecting portions of the posterior (in the back of the spine) bony elements and facet joints of the spine. This may also be referred to as a facet fusion.
Each type of spinal fusion has specific indications as well as specific risks and benefits, and may be done at more than one level of the spine.
The Role of Spinal Instrumentation in Multilevel Fusion
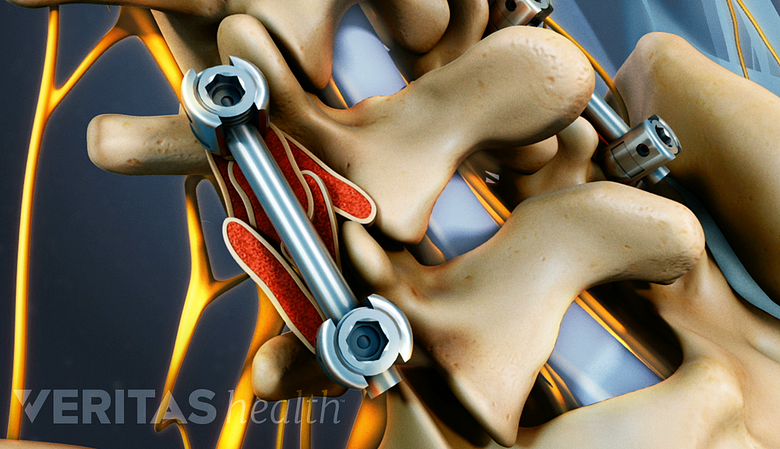
Spine fusion instruments stabilize and support the spine during the bone fusion process.
Most multilevel fusion procedures involve the use of spinal instrumentation in the back of the spine, but may also include supplemental anterior fixation. The role of spine fusion instrumentation is to provide additional spinal stability, acting as an internal brace while the bony fusion heals.
Common surgical implants used in multilevel spine fusion include spinal interbody cages, anterior plates, and posterior pedicle screws and rods, and sometimes hooks and wires.
Open Surgery vs Minimally Invasive Surgery
Both minimally invasive and standard open surgical techniques are used to fuse multiple levels of the spine. Open surgery typically provides more visibility and access to the surgical site, while the benefits of minimally invasive techniques include smaller incisions and a faster recovery period. Surgeons may choose either approach based on the indication and location of the surgery. Depending on the indication and surgical anatomy, an open or minimally invasive procedure may be preferred. These options should be discussed with the spine surgeon prior to agreeing on surgery.
Medical Clearance and Pre-Surgical Testing
Prior to any form of lumbar spine fusion, medical clearance is obtained, and patients who smoke and consume alcohol are strongly advised to cease. To prevent complications with post-surgical healing, surgeons typically advise patients to stop smoking at least 3 months before scheduling the surgical procedure. 2 Staartjes VE, de Wispelaere MP, Schröder ML. Improving recovery after elective degenerative spine surgery: 5-year experience with an enhanced recovery after surgery (Eras) protocol. Neurosurgical Focus. 2019;46(4):E7. doi:10.3171/2019.1.FOCUS18646 Patients will sometimes donate their own blood to be used at the time of surgery. More commonly, a machine (called the “cell saver”) is used during surgery to save lost blood and recycle it back to the patient, when the expected blood loss warrants it.
- 1 Mobbs RJ, Phan K, Malham G, Seex K, Rao PJ. Lumbar interbody fusion: techniques, indications and comparison of interbody fusion options including PLIF, TLIF, MI-TLIF, OLIF/ATP, LLIF and ALIF. J Spine Surg. 2015;1(1):2-18. doi:10.3978/j.issn.2414-469X.2015.10.05
- 2 Staartjes VE, de Wispelaere MP, Schröder ML. Improving recovery after elective degenerative spine surgery: 5-year experience with an enhanced recovery after surgery (Eras) protocol. Neurosurgical Focus. 2019;46(4):E7. doi:10.3171/2019.1.FOCUS18646